

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The presence of diastolic dysfunction has been previously documented in children in the acute phase of Kawasaki disease (KD).1)2)3) Diastolic dysfunction at the long-term follow-up in children with a history of KD (KDHx group) and coronary artery lesions (CALs) have also been reported.4) However, previously, left ventricular (LV) mass index or pulsed wave or tissue Doppler parameters such as the ratio of mitral inflow Doppler velocity during early diastole (E) and late diastole (A) (E/A) or mitral annular tissue Doppler velocity during early diastole (E´) was utilized to assess LV diastolic function.4) Pulsed-wave or tissue Doppler parameters are technically affected by angle dependency, 5) and also affected by movement of adjacent myocardial segments,6) thereby detection of subclinical diastolic dysfunction at long-term follow-up of children in the KDHx group by these parameters may be challenging.
With LV diastolic dysfunction, the resultant rise in left atrial (LA) pressure would lead to LA remodeling, reflected in impaired LA function.7) During systole, the LA functions as a reservoir of pulmonary venous return.8) LA reservoir function could be reflected in phasic LA volume changes such as LA total emptying fraction, which is (maximum LA volume - minimum LA volume) / maximum LA volume.8) Also, LA reservoir function could be assessed using myocardial deformation imaging as peak LA longitudinal strain (PLALS) at systole.9) In addition, LA stiffness index, which is defined as the amount of pressure required to change a unit of LA volume during the passive filling of LA,10) could be noninvasively obtained as E/E´/PLALS.11) An increased LA stiffness index reflects impaired LA reservoir function.12)13) In adults, LA total emptying fraction, PLALS, and LA stiffness index all have been utilized to assess the severity of LV diastolic dysfunction.7)11)14)15)
To date, LA reservoir function has not been evaluated at long-term follow-up in children in the KDHx group. Therefore, we assessed LA reservoir function at long-term follow-up of children in the KDHx group using LA total emptying fraction, PLALS, and LA stiffness index, along with conventional echocardiographic parameters, and compared it with those of a control group.
Methods
Study population
From 2007–2011, 487 children were admitted to CHA Bundang Medical Center for treatment of KD. Of these children, only the children with available long-term (≥ mean of 5 years after the acute phase of KD) follow-up echocardiograms were included in this study. The proposal for this study was approved by the Institutional Review Board of CHA University Bundang Medical Center (IRB: 2017-11-023), and since our study was retrospective, waiver of informed consent was obtained. At the time of admission, the diagnosis of KD was made according to the published American Heart Association (AHA) guidelines.16) For controls, data of children who were referred to the pediatric cardiology outpatient clinic for evaluation of chest pain and underwent echocardiography were retrospectively studied. Children who had structural heart anomalies or cardiac causes of chest pain were excluded from our study group.
Clinical data
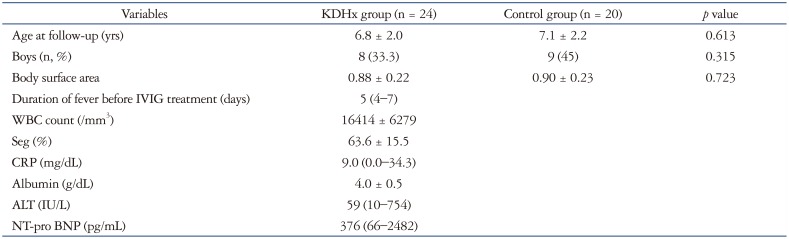
Data on duration of fever before intravenous immune globulin (IVIG) treatment were collected. Initial laboratory data obtained from a blood sample taken before IVIG treatment (white blood cell count, percentage of segmented neutrophils, serum albumin and alanine aminotransferase levels, C-reactive protein levels, and NT-pro B type natriuretic peptide levels) were also evaluated. All children in the KDHx group were administered IVIG (2 g/kg) at the acute phase of KD. Aspirin (80 mg/kg/day) was started with IVIG and was continued for 3–4 days after the child became afebrile, and the dose was reduced to 5 mg/kg/day and given for 6–8 weeks.16) IVIG nonresponders were defined as children experiencing persistent or recrudescent fever ≥ 36 h after completing the initial IVIG infusion.16) Exclusion criteria from the KDHx group were children who did not have late follow-up echocardiograms after the acute phase of KD.
Echocardiographic data
The long-term (≥ 5 years after the acute phase of KD) follow-up echocardiograms of children in the KDHx group were compared with those of the control group. All echocardiograms of the children in our study were obtained using a commercial echocardiography system (Acuson SC 2000, Siemens Medical, Mountain View, CA, USA). Both conventional echocardiography and myocardial deformational analyses were performed. Analysis of all conventional and deformation data were performed by a single pediatric cardiologist, who at the time of analysis was blinded to the group allocation of study subjects (KDHx versus control group).
Conventional echocardiography
Conventional echocardiographic parameters were obtained according to published recommendations.17) LV ejection fraction, E/A, E´, E/E´, and LV mass indexed to body surface area were obtained. The internal diameters of the proximal right coronary artery, proximal left anterior descending coronary artery, and left main coronary artery were measured. The definition of CALs were when calculated z-scores of the coronary arteries were ≥ 2.5 in one or more of the measured coronary sites.18) The z-scores of the coronary arteries were calculated according to the method of McCrindle et al.18) using the measured coronary dimensions and the published nonlinear regression equations.18)
Myocardial deformation analysis
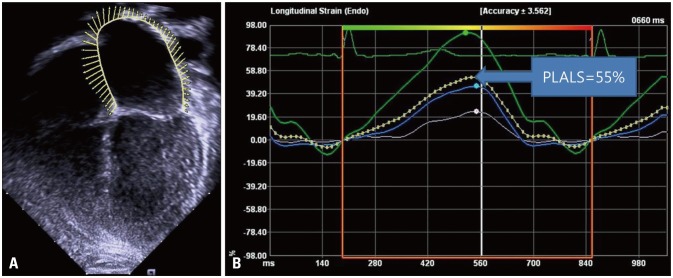
Two-dimensional echocardiographic images that were obtained at a mean of 70 frames per second and stored for prospective analysis were used for deformation imaging analysis. The software used for deformation analysis was velocity vector imaging (version 3.0, Siemens Medical). Three consecutive cardiac cycles were analyzed. PLALS, LV peak longitudinal systolic strain (ε), and LV peak systolic strain rate (SR) were all obtained offline using the apical four-chamber view. To obtain PLALS, the endocardial border of the LA was initially traced manually at the end of systole just before mitral valve opening.9)19) Subsequently, automatic tracking of the endocardial border of the LA using the velocity vector imaging software generated PLALS (Fig. 1A). The average of PLALS from the roof, interatrial septum, and the lateral wall of LA were used for analysis (Fig. 1B). LA stiffness index was obtained noninvasively by the formula E/E´/PLALS.11) The maximum LA volume, which was also generated automatically with PLALS by the velocity vector imaging software,20)21) was obtained and indexed to the body surface area. Using the maximum and minimum LA volumes automatically generated by the velocity vector imaging software, the LA total emptying fraction was calculated as (maximum LA volume - minimum LA volume) / maximum LA volume.8) To obtain LV peak longitudinal systolic ε and SR, the endocardial border of the LV was traced manually and tracked automatically by the software at the onset of the QRS wave on the electrocardiogram. The average of ε and SR curves from six segments (three from the interventricular septum and three from the LV free wall) were used for analysis.
Statistics
SPSS version 24 (IBM SPSS Statistics 24, Armonk, NY, USA) was used for data analysis. All data are expressed as mean ± standard deviation or median (range). Student's t-test or the Mann-Whitney U test, was used to compare continuous data between children in the KDHx and control groups. Chi-square analysis was used to compare categorical variables between the two groups. A p-value < 0.05 was considered significant. Correlation of LA total emptying fraction, PLALS, and LA stiffness index with clinical data was assessed by Pearson's or Spearman's correlation. To obtain intraobserver variability, one observer repeated an offline analysis of LA total emptying fraction, PLALS, LA stiffness index, LV longitudinal peak systolic ε, and SR in echocardiograms of 15 randomly selected children after 4 weeks. The intraobserver variability was evaluated by the mean percentage error.22)
Results
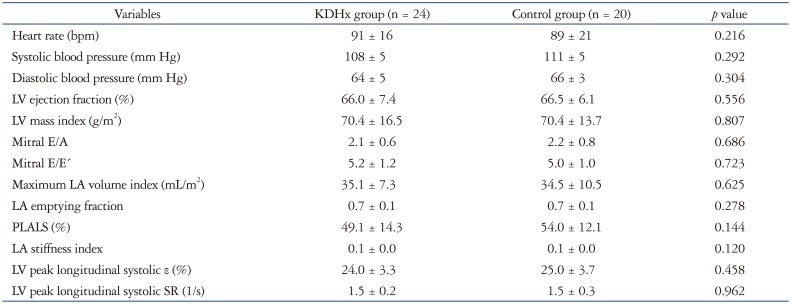
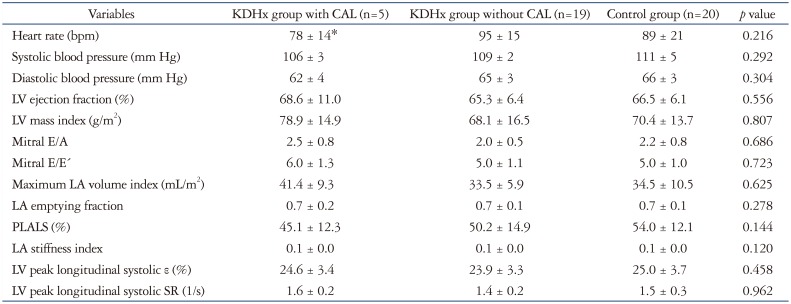
A total of 44 children were included in our study (24 in the KDHx group and 20 in the control group). The mean age and time from onset of KD to follow-up of the children in the KDHx group was 6.8 years and 5 years, respectively. Clinical and echocardiographic data of the children in the KDHx and control group are shown in Tables 1 and 2, respectively. Age at follow-up, percentage of boys, body surface area, heart rate, systolic and diastolic blood pressures were all similar between the children in the KDHx and control group. Six children (25%) showed incomplete KD. No children in our study were IVIG nonresponders. In the KDHx group, 5 children (20.8%) had CALs in the acute stage of KD. On echocardiograms performed at a mean follow-up period of 5 years after the acute phase of KD, no children showed CALs. As shown in Table 2, there were no significant differences in LV ejection fraction, LV mass index, mitral E/A, mitral E/E´, and maximum LA volume index between the children in the KDHx group at long-term follow-up and the control group. Likewise, there were no significant differences in LA emptying fraction, PLALS, LA stiffness index, LV peak longitudinal systolic ε, and SR between the children in the KDHx group at long-term follow-up and control group. In our study, LV systolic dysfunction was determined as LV peak longitudinal systolic ε < 18%, according to published reference values.23) No children in the KDHx group showed significant mitral regurgitation or LV systolic dysfunction. When the children in the KDHx group at long term follow-up was divided into subgroups according to initial CAL status at acute phase of KD, no significant differences were found in LA total emptying fraction, PLALS, LA stiffness index, LV peak longitudinal systolic ε, and SR among the children in the KDHx group with and without initial CAL at long term follow-up and control group (Table 3). No significant correlations were noted between LA emptying fraction, PLALS, LA stiffness index, and clinical and laboratory parameters. The mean percentage error for intraobserver variabilities in LA total emptying fraction, PLALS, LA stiffness index, LV longitudinal peak systolic ε, and SR were 16, 17, 18, 14, and 15%, respectively.
Discussion
We found no significant differences in LA reservoir function assessed by LA emptying fraction, PLALS, LA stiffness index, between the children in the KDHx and control groups. In addition, LV peak longitudinal systolic ε and SR were similar between the children in the KDHx and control groups. Since LA reservoir function reflects LV diastolic dysfunction,7)11)14)15) assessing LA reservoir function could determine the optimal follow-up intervals in children in the KDHx group, especially those without a history of CALs.
LA reservoir function could be assessed by LA total emptying fraction, PLALS, and LA stiffness index.8)12) Phasic changes of LA volume such as LA total emptying fraction have been shown to be associated with the severity of diastolic dysfunction.7) LA pressure increase due to elevated LV end-diastolic pressure may result in LA stretch and fibrosis, limiting the ability of LA filling and emptying.24)25) Acute LV diastolic dysfunction has been reported previously in children in the acute phase of KD.1)2)3) However, our results of similar LA emptying fraction between the children in the KDHx and control groups suggest that the LV diastolic dysfunction observed in the acute stage of KD may be resolved by the long term follow-up of KD.
PLALS has been shown to be more strongly correlated to LV diastolic function than tissue Doppler parameters26) in adults, due to strain (ε) and SR imaging being relatively independent of heart motion and nearby segment contraction.5)8)27) However, PLALS is known to be affected by significant acute mitral regurgitation,3) as acute mitral regurgitation could directly dilate the LA, independently of LV filling pressures.28) In addition, PLALS would decrease in the presence of LV systolic dysfunction, when impairment of mitral annular movement from the base to the apex in systole13) would decrease PLALS. In this study, no children in the KDHx group showed significant mitral regurgitation or LV systolic dysfunction. Therefore, in our study, we could assume that PLALS would reflect LV diastolic function, independent of the effects of significant mitral regurgitation or LV systolic dysfunction, and that LV diastolic function appear to be preserved.
Our study is the first to evaluate LA stiffness index derived by noninvasive methods11) at long term follow-up of children in the KDHx group and controls. In adults, LA stiffness index has been shown to be able to distinguish diastolic heart failure from diastolic dysfunction.11) Also, in adult atrial fibrillation patients undergoing LA ablation, LA stiffness index has been shown to estimate the compliance of the LA myocardium because it is the ratio of change in volume to change in pressure during LA passive filling.10) Our results of similar LA stiffness index in the children in the KDHx and control groups at long term follow-up suggest that LA compliance may be normalized by long term follow-up of KD.
Previously, LV diastolic dysfunction detected during the long-term follow-up of children in the KDHx group had been studied with conflicting results. Both structural abnormalities4)29) and functional impairment30)31) of coronary arteries have been associated with diastolic dysfunction in children in the KDHx group. Arnold et al.29) identified diastolic abnormalities in segments supplied by stenotic coronary arteries in 17 children in the KDHx group who had CALs. Selamet Tierney et al.4) showed the association of coronary abnormalities with diastolic dysfunction using evidence of prolonged deceleration time and decreased E´ velocity on follow-up of children in the KDHx group and coronary abnormalities. Additionally, decreased coronary flow reserve in children in the KDHx group without overt coronary structural abnormalities have been reported.30)31) Based on these observations, we could speculate a subclinical decrease in LV myocardial function and resulting atrial remodeling leading to altered LA reservoir function in children in the KDHx group due to the functional impairment of coronary arteries. However, the results in this study did not show significant differences in LA reservoir function, LV peak longitudinal systolic ε, and SR in the children in the KDHx and control groups. Possible explanations of this similar outcomes between the two groups may be the small number of the study population, or the limited number of children with CALs in the KDHx group at the acute phase of KD (5/24, 16.7%).
Another reason for the similar LA reservoir function and LV peak longitudinal systolic ε and SR at long term follow-up in the children in the KDHx and control groups may be that LV diastolic dysfunction may be more evidently detected in the acute phase of KD (less than 1 month of onset of KD)4) than in the later stages of the disease. In the acute stage of KD, myocarditis may cause myocardial interstitial edema,2) resulting in LV diastolic dysfunction. However, in the convalescent phase, normalization of echocardiographic parameters such as mitral E/A and E/E´, have been reported.1) Histologic abnormalities in the follow-up period of KD, such as inflammatory cell infiltration, interstitial fibrosis, and disarray have been shown in specimens of KD patients with giant aneurysms.32) However, to date, it is unclear whether myocarditis in the acute stage of KD causes myocardial dysfunction at long-term follow-up of KD, independent of CALs.33) Resolution of acute LV systolic dysfunction in children in the KDHx group 1–3 years after KD onset have been reported.34) Our results suggest that LV diastolic function also may be normalized in the long-term follow-up of children in the KDHx group without CALs, as implied previously.33)
Limitations
Limitations of this study are the retrospective design, the small number of subjects in the study population which might have affected our statistical results, and the unavailability of invasive hemodynamic data as a reference value for assessment of LV diastolic function. However, since children in the KDHx group at long-term follow-up were clinically asymptomatic, invasive cardiac catherization was not necessary, as previously stated.16) In addition, all deformation analyses were performed using the apical four-chamber view only, and the limited number of analyzed segments might have affected our statistical results.
 XML Download
XML Download