

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
In preterm infants, a hemodynamically significant patent ductus arteriosus (hsPDA) has been shown to be associated with increased mortality1) and can cause severe morbidities, such as intraventricular hemorrhage (IVH) and necrotizing enterocolitis (NEC). However, the benefits of treatment to close an hsPDA in preterm infants have been challenged,2) and evidence has indicated that early routine treatment to close an hsPDA in the first 2 weeks after birth does not improve long-term neonatal outcomes, such as IVH and bronchopulmonary dysplasia (BPD).3) Recently, a study advocated the “nonintervention” approach for an hsPDA, focusing on the negative consequences of indomethacin use, such as NEC and intestinal perforation.4) However, unlike neonatal outcomes, the impact of different responses to medical treatment for an hsPDA on outcomes of left ventricular (LV) function in preterm infants has not been appropriately studied.
An hsPDA in preterm infants is known to increase preload, resulting in an increase in LV output.5) The effect of an hsPDA on LV function in preterm infants beyond the neonatal period has been studied;6)7) however, the impact of different responses to medical treatment for an hsPDA on LV strain has not been assessed. In an animal study, remodeling of the LV was observed in immature hearts,8) which could result in potential LV systolic dysfunction (LVSD). It is unclear whether prolonged exposure to an hsPDA can contribute to this remodeling of the LV in preterm hearts. Myocardial strain, which describes changes in the length of myocardial fibers and is expressed as a percentage,9) has been applied to detect myocardial dysfunction in neonates.10) Myocardial strain could be obtained by velocity vector imaging, which utilizes speckle and endocardial contour tracking to assess regional and global cardiac function.11) We speculated that strain parameters by velocity vector imaging, namely, LV longitudinal peak systolic strain (ε), could sensitively detect potential LVSD among preterm infants who have undergone medical or surgical treatment for hsPDA.
Therefore, we aimed to investigate the outcomes of LV function according to different responses to medical treatment for an hsPDA in preterm infants by analyzing LV longitudinal peak systolic ε at term-equivalent age.
Methods
Study population
We retrospectively assessed the clinical and echocardiographic data of 21 preterm infants born at gestational age (GA) < 31 weeks who were admitted to the neonatal intensive care unit of CHA Bundang Medical Center from January 2012 to December 2013. Exclusion criteria for this study were infants with congenital heart defects except for a small patent foramen ovale. The proposal for this study was approved by the Institutional Review Board of CHA University Bundang Medical Center, and the requirement for patient consent was waivered because the study was a retrospective one (IRB No. 2017-08-031).
Definition of an hsPDA and treatment groups
Initial echocardiograms of all infants in our study group were obtained within postnatal day 3 to assess the presence of hsPDA. An hsPDA was defined as a PDA > 2 mm in transductal diameter with an unrestrictive left-to-right shunt through the PDA and pulmonary hemorrhage, or PDA > 2 mm in diameter and cardiomegaly and pulmonary edema on chest X-ray with one of the following: respiratory failure requiring the increase in ventilator settings, or hypotension requiring vasopressors.12)
The “medication” group included infants with hsPDA who were treated with ibuprofen (intravenously, one cycle comprising an initial dose of 10 mg/kg, and two consecutive doses of 5 mg/kg each 24 hours apart) or indomethacin (intravenously, an initial dose of 0.2 mg/kg along with 0.1 mg/kg 12 hours later and 0.1 mg/kg 24 hours later) at the diagnosis of the hsPDA at postnatal day 2–3. These infants underwent follow-up echocardiography after each medication cycle until documentation of closure of the hsPDA. None of the preterm infants in this group received prophylactic treatment (medical treatment within 12 hours after birth)13) for their hsPDA.
The “no-hsPDA” group included preterm infants who did not show a PDA at initial echocardiography within postnatal day 3 or who initially had a PDA which did not meet the hsPDA criteria. Serial echocardiography was performed 2 days later, and if the PDA closed spontaneously or reduced in size, no treatment was administered.
The “ligation” group included infants who, after experiencing medical treatment failure, continued enteral feeding but cardiopulmonary compromise continued, as previously described as the “conservative approach” to PDA ligation.14)
Neonatal risk factors and outcomes
The prevalences of grade ≥ III (ventricles filling with distension) IVH15) and grade ≥ IIA NEC according to the modified Bell's staging criteria16) were evaluated. Infants were classified as having Grade IIA NEC when systemic symptoms such as temperature instability, apnea, or bradycardia were present, intestinal symptoms such as absent bowel sounds with or without abdominal tenderness were found in addition to bright red blood from rectum, and radiological signs such as intestinal dilation, ileus, or pneumatosis intestinalis were found. BPD was defined as the requirement of supplemental oxygen at 36 weeks GA.
Echocardiographic data
All echocardiograms analysed for this study were obtained at a mean of 40 weeks corrected age (term equivalent age) using commercially available ultrasound equipment (Acuson SC 2000, Siemens Medical, Mountain View, CA, USA).
Conventional echocardiographic parameters
The PDA diameter was measured at the pulmonary end. Maximal tricuspid regurgitation (TR) jet velocity from continuous- wave Doppler was obtained to estimate right ventricular systolic pressure derived from the modified Bernoulli equation (TR jet velocity2 × 4).17)18)19) Maximal TR jet velocity, LV ejection fraction, mitral inflow Doppler velocity during early diastole (E), mitral annular tissue Doppler velocity during early diastole (E′), and the ratio of mitral E/E′ was obtained according to previous recommendations.19) The isovolumic contraction time (IVCT) and isovolumic relaxation time (IVRT) were calculated from tissue Doppler imaging,19) and the LV myocardial performance index (MPI) was calculated as follows20): LV MPI = (IVCT + IVRT)/LV systolic ejection time.
Myocardial deformation analysis
Using velocity vector imaging software (version 3.0, Siemens Medical), digital images previously obtained at 70 frames per second (fps) and stored were analyzed. Two investigators blinded to the clinical characteristics of the study population performed all offline analyses.
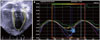
In the apical four-chamber view, endocardial border of the LV at the onset of the QRS wave was traced manually and subsequently tracked automatically by the velocity vector imaging software to acquire LV longitudinal peak systolic ε.21) ε curves were derived from six segments (three from the LV free wall and three from the interventricular septum), and LV longitudinal peak systolic ε was identified as the highest point of the average of the six curves (Fig. 1).21) Three cardiac cycles were analyzed and averaged. Representative examples of LV longitudinal peak systolic ε at term-equivalent age in the three groups according to treatment of hsPDA are shown in Fig. 2.
Statistical analysis
All values are expressed as mean ± standard deviation or median (minimum-maximum range), as appropriate. Data were analyzed using SPSS version 24 (IBM SPSS Statistics 24, IBM Corp., Armonk, NY, USA). Continuous data between two groups were analyzed using Student's t-test or the Mann-Whitney U test, as appropriate, and data among three groups were analyzed using the Kruskal-Wallis test. Categorical variables were analyzed using chi-square analysis. A p-value < 0.05 was considered significant. Pearson's or Spearman's correlation was used, as appropriate, to determine correlations between variables. For intraobserver variability, one observer performed an offline repeat analysis of LV longitudinal peak systolic ε in 15 infants after an interval of 4 weeks. For interobserver variability, two independent observers, blinded to the clinical data of the infants at the time of analysis, performed a separate analysis of LV longitudinal peak systolic ε in 15 infants. Intraobserver and interobserver variabilities were calculated as the mean percentage error.22)
Results
Demographic and clinical data of the three groups are shown in Table 1. GA, birth weight (BW), age and weight at echocardiography were similar among the three groups. No patients in our study were small for GA (BW ≤ 10% for GA). In the medication group, 3 patients (50%) received 1 treatment cycle, 2 patients (33.3%) received 2 treatment cycles, and 1 patient (16.7%) received 3 treatment cycles. The median medical treatment duration was 4.5 days (range, 2–9 days). In the ligation group, 1 patient (11.1%) received 1 treatment cycle, 7 patients (77.8%) received 2 treatment cycles, and 1 patient (11.1%) received 3 treatment cycles. In the ligation group, the median medical treatment duration was 6 days (range, 3–9 days), and the median postnatal age at surgery was 20 days (range, 9–31 days). The median delay from medical treatment failure to ligation was 9 days (range, 6–18 days). None of the patients in the ligation group experienced postligation cardiac syndrome23) that required milrinone treatment. In the ligation group, 3 patients experienced NEC; 1 patient showed NEC at postnatal 3 days, and 2 patients experienced NEC at 14 days and 60 days after ligation, respectively. Additionally, no patient underwent surgical treatment for NEC. In contrast, all patients in the medication group had either PDA closure or reduction in the PDA size to below hemodynamic significance before 2 weeks of postnatal age.
The echocardiographic data of preterm infants are shown in Table 2. No differences in conventional echocardiographic parameters were observed among the three groups. LV longitudinal peak systolic ε was significantly decreased in the ligation group compared to that in the medication group or no-hsPDA group. There were no differences in LV longitudinal peak systolic ε between the medication and no-hsPDA groups. We defined LVSD as LV longitudinal peak systolic ε < 18%,24) and found that 55.6% (5/9) of infants in the ligation group had LVSD at term-equivalent age, while 16.7% (1/6) of infants in the other groups had LVSD.
When the preterm infants in our study were divided into subgroups according to adverse neonatal outcomes, LV longitudinal peak systolic ε was significantly decreased in patients who experienced NEC compared to those who did not experience NEC (14.3 ± 3.6% vs. 20.1 ± 3.4%, p = 0.017).
Discussion
We found that the PDA ligation group had the worst outcomes of LV function at term-equivalent age as shown by decreased LV longitudinal peak systolic ε when compared to the outcomes in the medication and no-hsPDA group. However, LV longitudinal peak systolic ε did not differ between the medication and no-hsPDA groups. Among the neonatal outcomes, only the prevalence of NEC showed a significant negative correlation with LV longitudinal peak systolic ε.
To our knowledge, this is the first study to compare LV systolic function by LV longitudinal peak systolic ε according to different responses to medical treatment for a PDA. Previous studies on the outcome of different responses to medical treatment for a PDA have focused on the prevalence of BPD and neonatal outcomes.4)14) Our study is unique in that we analyzed outcomes of LV function at term-equivalent age in preterm infants who were treated for an hsPDA according to different responses to medical treatment. Previous studies on the effects of PDA on LV function focused on the immediate postoperative period after PDA ligation,25)26) did not take into account different responses to medical treatment for an hsPDA,6) or compared term infants as controls.27)
Feasibility of myocardial deformation imaging as a measure of LV systolic function in neonates
Myocardial ε has been reported to be a more sensitive parameter than conventional echocardiographic parameters for the detection of early myocardial dysfunction in children.28) Additionally, in neonates, ε has been utilized in myocardial functional evaluation.29)30) In our study, although LV longitudinal peak systolic ε was significantly decreased in the ligation group compared to other groups, no differences in conventional echocardiographic parameters were found among the three groups. ε can be obtained by tracking along the direction of the ventricular wall and not along the ultrasound beam; therefore, it has been reported to be less angle dependent than tissue Doppler parameters, such as mitral valve E/E′.31)32) Based on our findings, we speculate that LV longitudinal peak systolic ε would enable a sensitive detection of subtle LVSD that may be present in preterm infants treated for an hsPDA.
Reasons for decreased LV longitudinal peak systolic ε in the ligation group
We speculate that one reason for the decreased LV longitudinal peak systolic ε at term-equivalent age in the ligation group compared to that in the other treatment groups in our study was the higher percentages of infants below 28 weeks GA and those with BW < 1000 g in the ligation group. A higher risk of decreased LV systolic function immediately after PDA ligation in preterm infants weighing < 1000 g26) has been reported. Altered loading conditions, such as acute increase in systemic vascular resistance,25)26) occurs immediately after PDA ligation and could cause LV dysfunction in this period.25)26) As the ligation group in our study had more premature infants < 28 weeks GA, the myocardium in the ligation group would be more immature and more intolerant to changes in afterload.33) We speculate that in our study, in the ligated group, subtle myocardial dysfunction initiated at the time of surgical ligation, which coincided with sudden changes in preload and systemic vascular resistance25)26)34) may have persisted to term-equivalent age, presenting as decreased LV longitudinal peak systolic ε in this group.
Another reason for the decreased LV longitudinal peak systolic ε at term-equivalent age in the ligation group in our study may be prolonged preload exposure due to an hsPDA at the immature myocardium. In our study, PDA ligation was performed using the “conservative approach,” indicating treatment only after failure of initial medical treatment for the hsPDA, and symptoms of pulmonary overcirculation or systemic hypoperfusion persisted.14) Additionally, in our study, after medication failed to close the hsPDA, there was a delay before ligation. A delay in surgery has been reported to lower ligationassociated morbidities,14) however, none of our patients experienced postligation cardiac syndrome23) that required milrinone treatment. On the other hand, this delay resulted in prolonged preload exposure, thereby presumably accelerating LV remodeling in the ligation group. Neonatal outcomes, namely BPD and death, have been associated with prolonged exposure to an hsPDA in preterm infants undergoing PDA ligation.35) We speculate that shortening exposure to an hsPDA may be beneficial for preserving LV systolic function at termequivalent age in preterm infants. Our results support the need for selection criteria for the early detection of preterm infants at high risk of medical treatment failure of an hsPDA.5) In our study, preterm infants in the ligation group underwent ligation at a mean of 3 weeks postnatal age. Based on our results, we speculate that earlier PDA ligation than a mean of 3 weeks postnatal age might be associated with better cardiovascular outcomes in preterm infants. Further studies involving a larger group of patients will be needed to validate this assumption.
Preserved LV function in the medication group at term-equivalent age
Recently, medical and surgical treatment rates for an hsPDA in preterm infants have been declining.36) The treatment strategy for an hsPDA has been challenged by “nonintervention” approaches, namely management with ventilator manipulations and diuretics only.4) Reportedly, no benefits with regard to neonatal outcomes were found in the medical or surgical treatment group when compared to the outcomes with the nonintervention approach.4) However, in our study, when initial medical treatment was administered at 2–3 days postnatal age, LV systolic function in the medication group at termequivalent age was comparable to that in the no-hsPDA group. Additionally, as previously reported,37) the duration of mechanical ventilation or other important neonatal morbidities, such as NEC and BPD, did not differ between the medication and no-hsPDA groups in our study. Importantly, adverse reactions of indomethacin for PDA treatment have included immediate impairment in myocardial deformation with partial subsequent recovery 1 hour later, owing to alterations in coronary flow and resistance.38) However, we speculate that no persistent effects of indomethacin infusion affected LV systolic function in our study, as at term-equivalent age, no difference in LV longitudinal peak systolic ε was noted between the medication and no-hsPDA groups. Additionally, the medication group showed better preserved LV longitudinal peak systolic ε compared to the ligation group in our study, and the main difference between the two groups was the duration of ductal patency. Therefore, our results support the hypothesis that prolonged hsPDA may cause adverse outcomes.3) Based on our results, we speculate that in preterm infants with an hsPDA, early PDA ligation at less than 20 days of postnatal age in cases of medical treatment failure would be beneficial for preserving LV systolic function.
Analysis of LV longitudinal peak systolic ε according to adverse neonatal outcomes
In our study, LV longitudinal peak systolic ε was significantly decreased in patients who experienced NEC compared to those who did not experience NEC. Only infants in the ligation group showed NEC. In addition to quantitative assessment of “ductal steal” as documented by the ratio of celiac artery blood flow to LV output in preterm infants with an hsPDA,39) an hsPDA has been reported to be an independent risk factor for the development of NEC, while therapy with indomethacin was not significantly associated with the risk for NEC.40) Therefore, we speculate that longer duration of an hsPDA in the ligation group might have contributed to the higher prevalence of NEC.
Limitations
Our study was a retrospective observational study. Therefore, we could not establish causality. The small numbers of patients in our subgroups may have limited our statistical results. There were no preterm infants who received prophylactic indomethacin or infants who had an hsPDA but did not receive treatment for the hsPDA in our study. Therefore, we could not compare the outcome of those approaches.



 XML Download
XML Download