

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Type 1 diabetes (T1D) mellitus is one of the most common endocrine and metabolic conditions in childhood.1) In Egypt, its incidence is 8/100000 per year in children under the age of 15 years.2)
Studies on adults have reported that patients with T1D show ultra-structural and functional myocardial deterioration.3) Similarly, it has been reported that young patients with T1D have significant changes in left ventricular dimension and myocardial relaxation.4) Diabetic cardiomyopathy (DCM) as a distinct clinical entity continues to be the subject of debate since it was first introduced by Rubler et al.5) in 1972. By definition, DCM is a distinct primary disease process which develops secondary to a metabolic insult, resulting in structural and functional abnormalities of the myocardium leading to heart failure. 6) The most frequent and earliest detectable functional abnormality in DCM is impaired diastolic function.7) The early reductions in diastolic performance have been found to be followed by progressive reductions in systolic function during the later stages of DCM.8)
Echocardiography is a non-invasive method that can be used for the diagnosis of DCM or diabetes induced myocardial dysfunction. Tissue Doppler echocardiography is a modality of echocardiography which proved to have additional value in the evaluation of ventricular filling in diabetic patients.3)
Conventional and tissue Doppler echocardiography can predict early stages and progression of diabetic cardiac changes.9)
However, studies which evaluated the use of tissue Doppler in detection of cardiac dysfunction in children with T1D are few and conflicting.
The aim of the present study is to assess right and left ventricular functions using conventional and tissue Doppler echocardiography in children and adolescents with T1D.
Methods
Study design
This cross sectional study included 40 patients (age between 6 and 16 years) with T1D and receiving insulin injection for duration more than 5 years and 42 controls matched for age and sex. Patients with signs of major complications such as renal, retinal or neurological disease were excluded. Patients with concomitant illness affecting cardiac function, medications known to affect cardiac functions or those with congenital heart disease were also excluded from the study. The controls were volunteers, friends, or neighbors of patients, workers or nurses in the hospital. They were matched prospectively for age, gender, and body mass index (BMI). Full physical examination including cardiac examination and blood pressure (BP) measurement, as well as echocardiography performed before recruiting them to ensure that they do not have an underlying cardiac problem. Informed consent was obtained from all included patients and controls. The study was approved by the Institutional Ethical Committee.
Methodology
Clinical evaluation
All children fulfilling the inclusion criteria were subjected to full history taking including: cardiac manifestations (history of palpitation, chest pain, hypertension and exertion on exercise and manifestations of heart failure), dietary habits, exercise habits and efforts to modify life style habits. Thorough clinical examination was performed. BP measurement (supine, sitting, and standing for detection of autonomic dysfunction). The measurements were plotted on the BP percentiles of BP of children. 10) Body weight (kg) and height (m) to calculate BMI (kg/m2) were measured and percentiles were assessed using Egyptian growth curves.11) Thorough cardiac examination was performed to detect cardiomegaly or manifestations of heart failure.
Laboratory evaluation
Glycosylated hemoglobin A1c (HbA1c), serum total cholesterol (TC), triglycerides (TG), low density lipoproteins (LDL) cholesterol and high density lipoproteins (HDL) cholesterol were measured for all patients. In nondiabetic patients, HbA1c is usually < 6%, whereas in diabetic patients, values of 6–7.9% represent good metabolic control; values of 8–9.9% represent fair metabolic control; and values of HbA1c ≥ 10% represent poor metabolic control.12) Dyslipidemia was defined by the American Diabetes Association13) as having LDL-cholesterol > 100 mg/dL, HDL-cholesterol < 40 mg/dL (males) and < 50 mg/dL (females), TC > 200 mg/dL and TG > 150 mg/dL; and dyslipidemia was considered present if one or more of these lipid or lipoprotein levels are abnormal.14)
Electrocardiography
Twelve leads electrocardiography was performed for assessment of heart rate, rhythm, P-R interval and corrected Q-T interval.
Echocardiography & tissue Doppler study
Echocardiography was performed for all cases and controls in the supine, left lateral position using General Electric (GE, Vivid-5, Horton, Norway) system with probe 3 or 5 MHz (multi-frequency transducer) according to the age of patient, having tissue velocity imaging capabilities.
The electrocardiography cable was connected to the ultrasound machine to define and to time the cardiac cycle events. The examination was performed by a pediatric cardiologist expert in echocardiography and tissue Doppler imaging (TDI) in accordance with the recommendations of the American Society of Echocardiography.15)
The examination consisted of M-mode, two dimensional, pulsed-wave, and color Doppler blood flow velocity measurements of the heart valves. Trans-mitral and trans-tricuspid flows were obtained with pulsed wave Doppler at the leaflet tips; early diastolic inflow velocity (E), velocity during active atrial contraction (A), E to A wave (E/A) ratio, and deceleration time were measured.
TDI was obtained from the four chambers apical view, and tissue velocities were calculated. Using pulsed tissue velocity indices, the sample volumes were placed in the lateral sides of the mitral and tricuspid annuluses and the base of the interventricular septum (IVS). The peak systolic and early and late diastolic velocities (E′ and A′, respectively) at these points were measured, and the E/E′ ratio was calculated. The isovolumic relaxation time (IVRT) and isovolumic contraction time (IVCT) were both measured for both left ventricle (LV) and right ventricle (RV) lateral walls.
Calculation of global myocardial performance index (MPI) was performed by pulsed tissue velocity imaging. For tissue Doppler, all interval measurements were performed within one cardiac cycle. The MPI was calculated a′–b′/b′ where a′ is the time interval from the end of A′ wave to the onset of E′ wave and b′ the time from the onset to the end of the S′ wave.
To reduce the effect of respiration on tissue velocities and as breath holding was not applicable in young children, three cardiac cycles were, recorded, and the average velocity was calculated. To reduce intraobserver variability three different measurements for each tissue Doppler index was done and the average was taken.
Left ventricular parameters were assessed and grading of LV and RV diastolic dysfunction (DD) were performed.15)16)
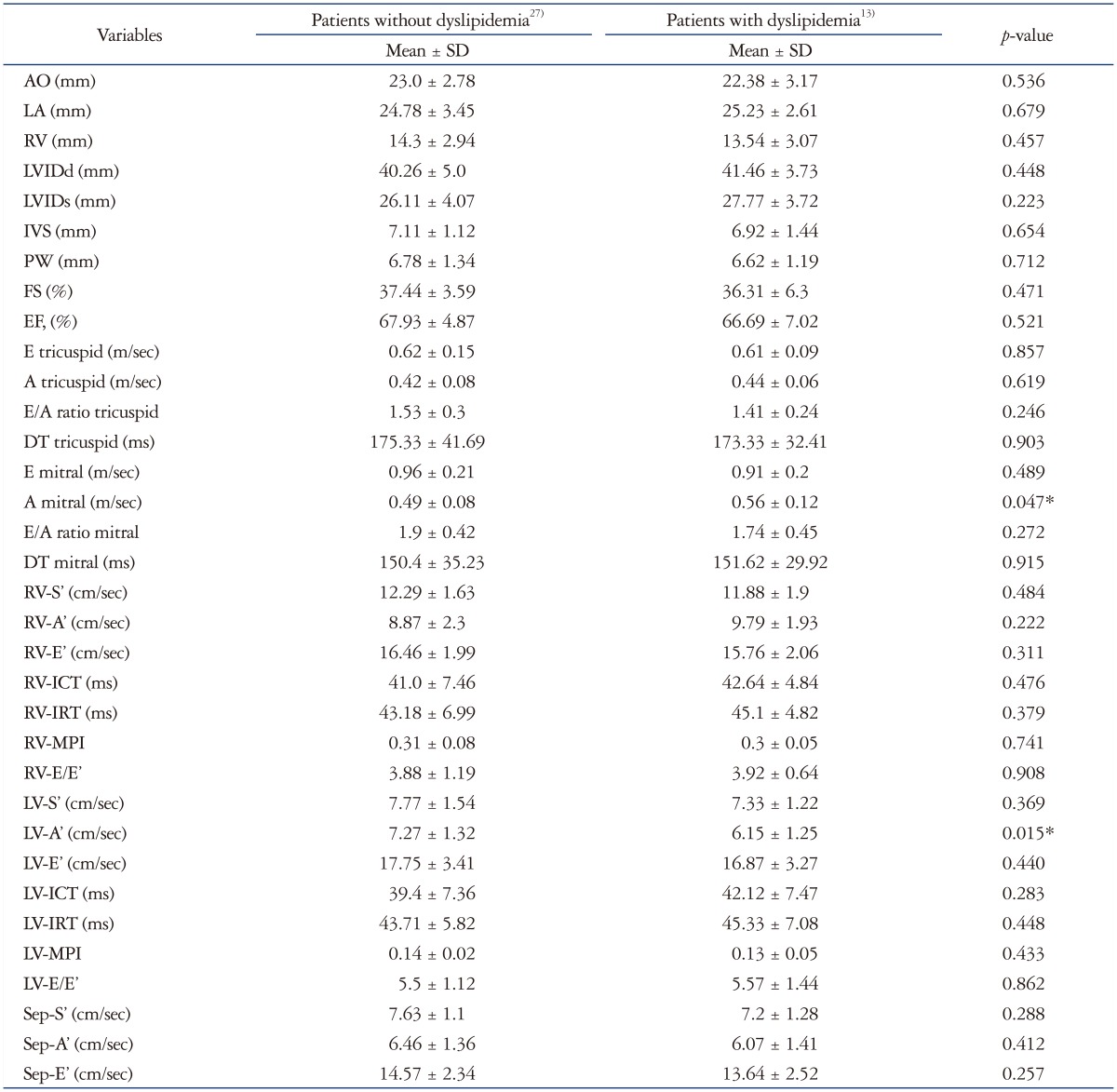
The patients were divided into two groups according to presence of dyslipidemia and compared according to their echocardiographic data to find any effect of dyslipidemia on cardiac echo parameters.
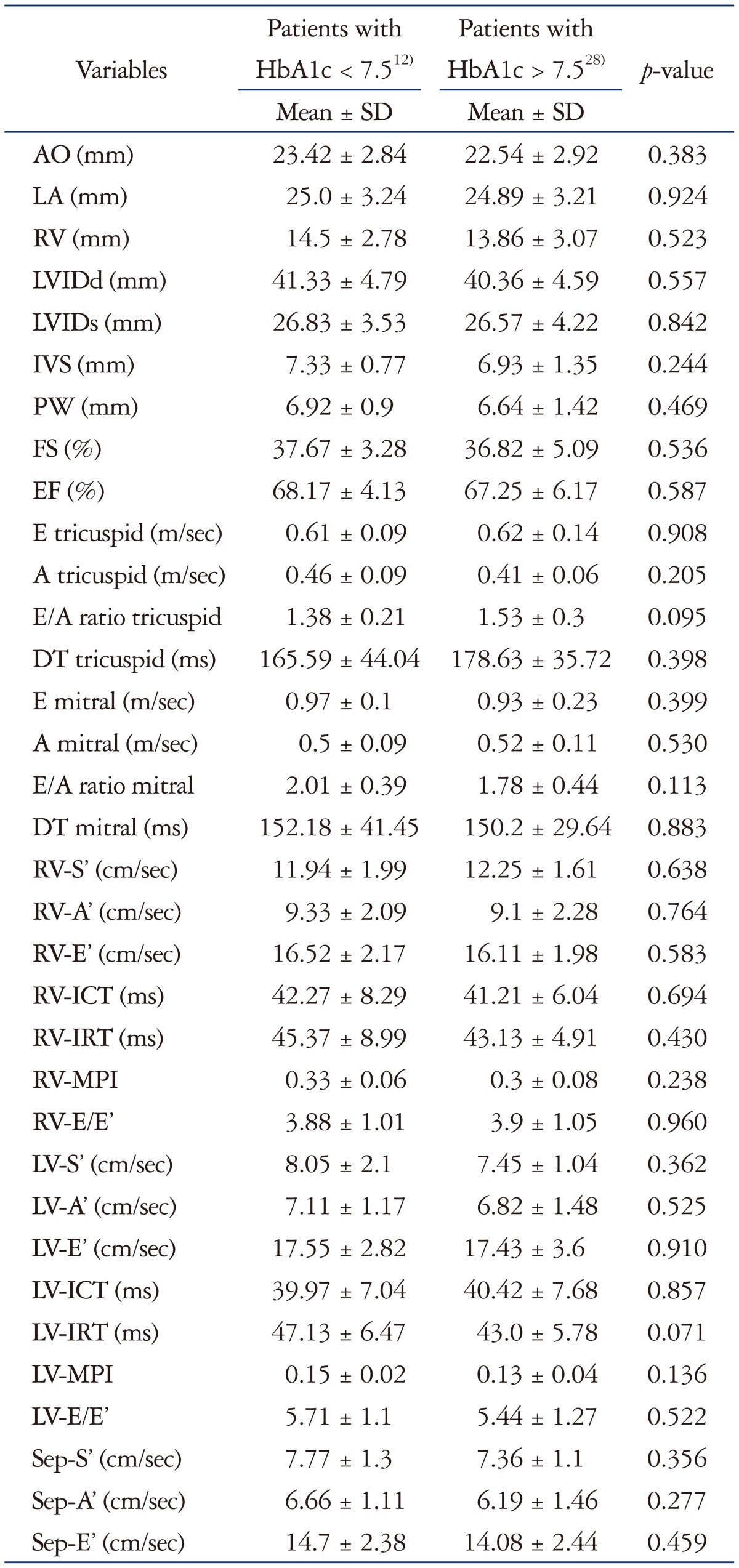
The patients were also divided into two groups according to their glycosylated HbA1c level and compared according to their echocardiographic data to find any effect of degree of glycemic control on cardiac echo parameters.
Correlations were done between the level of HbA1c, duration of diabetes and level of TG and the parameters of DD.
Statistical analysis
Data were statistically described in terms of mean ± standard deviation (SD), median and range, or frequencies (number of cases) and percentages when appropriate. Comparison of numerical variables between the study groups was done using Student t test for independent samples when data were normally distributed and Mann Whitney U test for independent samples when not normally distributed. For comparing categorical data, chi square (χ2) test was performed. Exact test was used instead when the expected frequency is less than 5. p values less than 0.05 was considered statistically significant. All statistical calculations were done using computer program Statistical Package for the Social Science (SPSS Inc., Chicago, IL, USA) release 15 for Microsoft Windows (2006).
Results
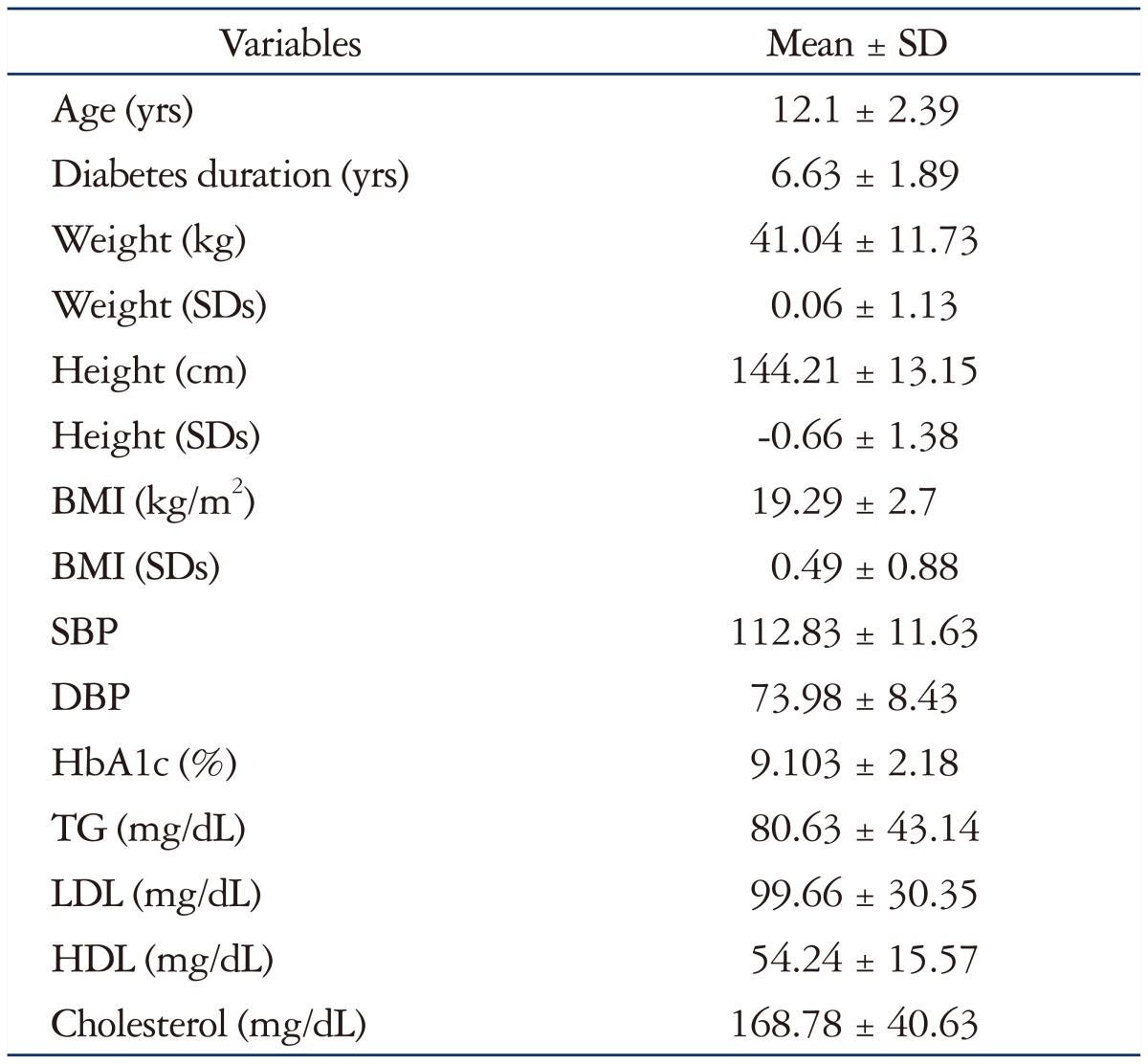
The mean age ± SD of the patients was 12.1 ± 2.39 versus 11.6 ± 1.23 for the controls (p value 0.235). The diabetes data of the patients included in this study are shown in Table 1 as well as the comparison between the patients and controls regarding the clinical data. None of our patients had cyanosis, palpitation or dyspnea at rest but there was 17.5% with exercise intolerance. Only a 16-year-old female patient with BMI26) and dyslipidemia had BP above 95th percentile. All patients had normal cardiac examination and normal cardio autonomic tests. There was positive family history of diabetes in 42.5% of the patients. All the patients were receiving insulin.
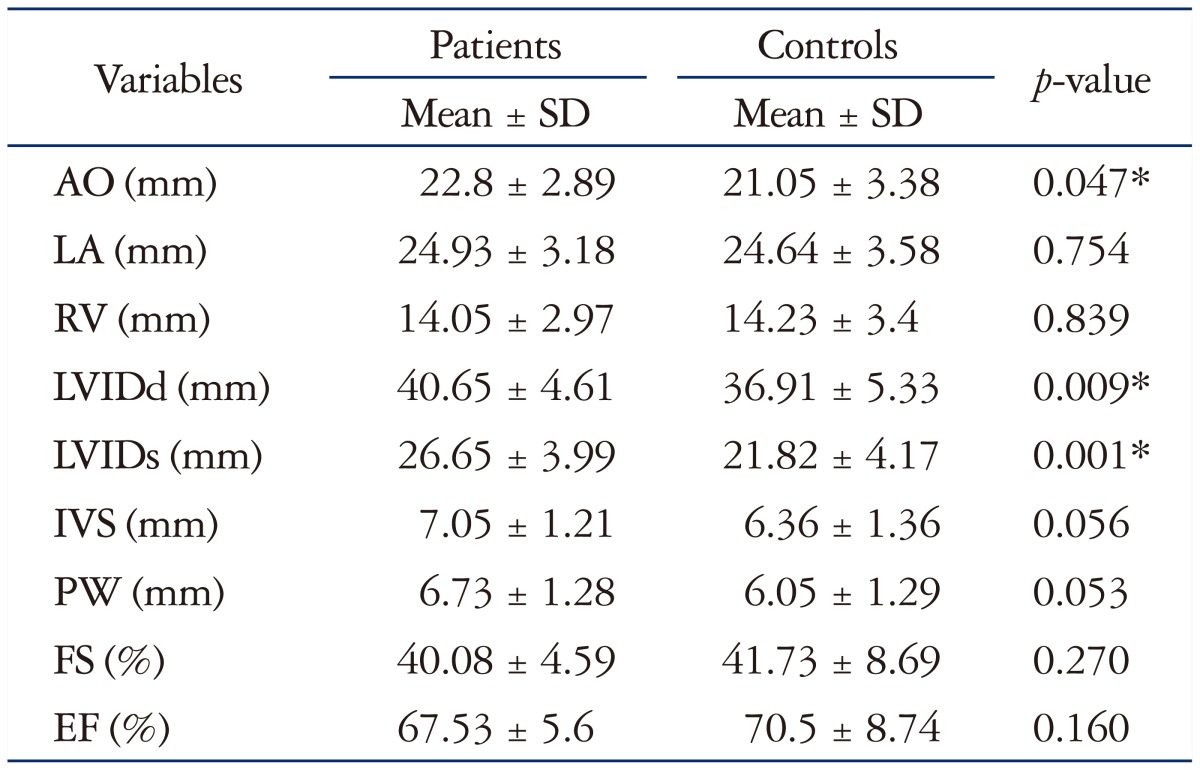
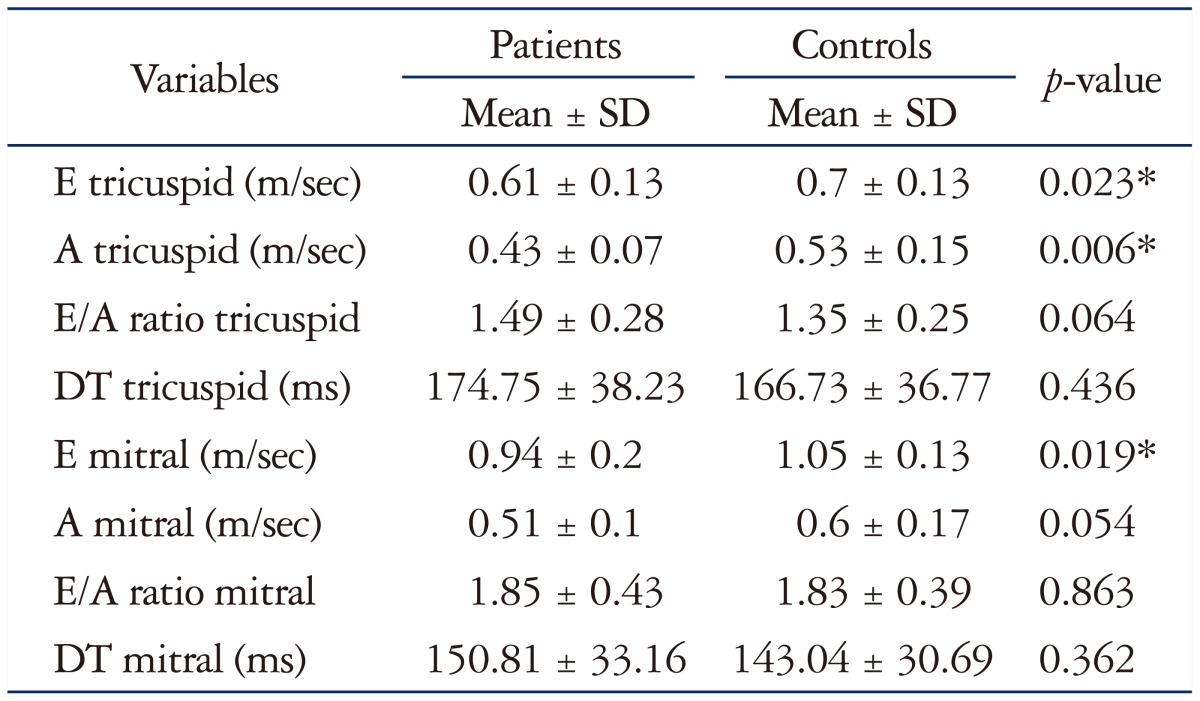
Table 2 shows comparison between M-mode echocardiographic data of patients and controls. Dimensions of aorta, left atrium (LA), IVS, left ventricular posterior wall (LVPW), left ventricular internal diameter in diastole (LVIDd) and left ventricular internal diameter in diastole (LVIDs) were significantly higher in diabetic patients compared to controls (p value 0.000, 0.025, 0.000, 0.002, 0.000, and 0.000, respectively). The fractional shortening (FS) was significantly lower in cases than controls (p value 0.033). Doppler echocardiographic study showed that the patients had significantly lower E and A waves velocity across both the tricuspid valve and the mitral valve than controls (p value 0.000, 0.000, 0.006, and 0.000, respectively) as shown in Table 3.
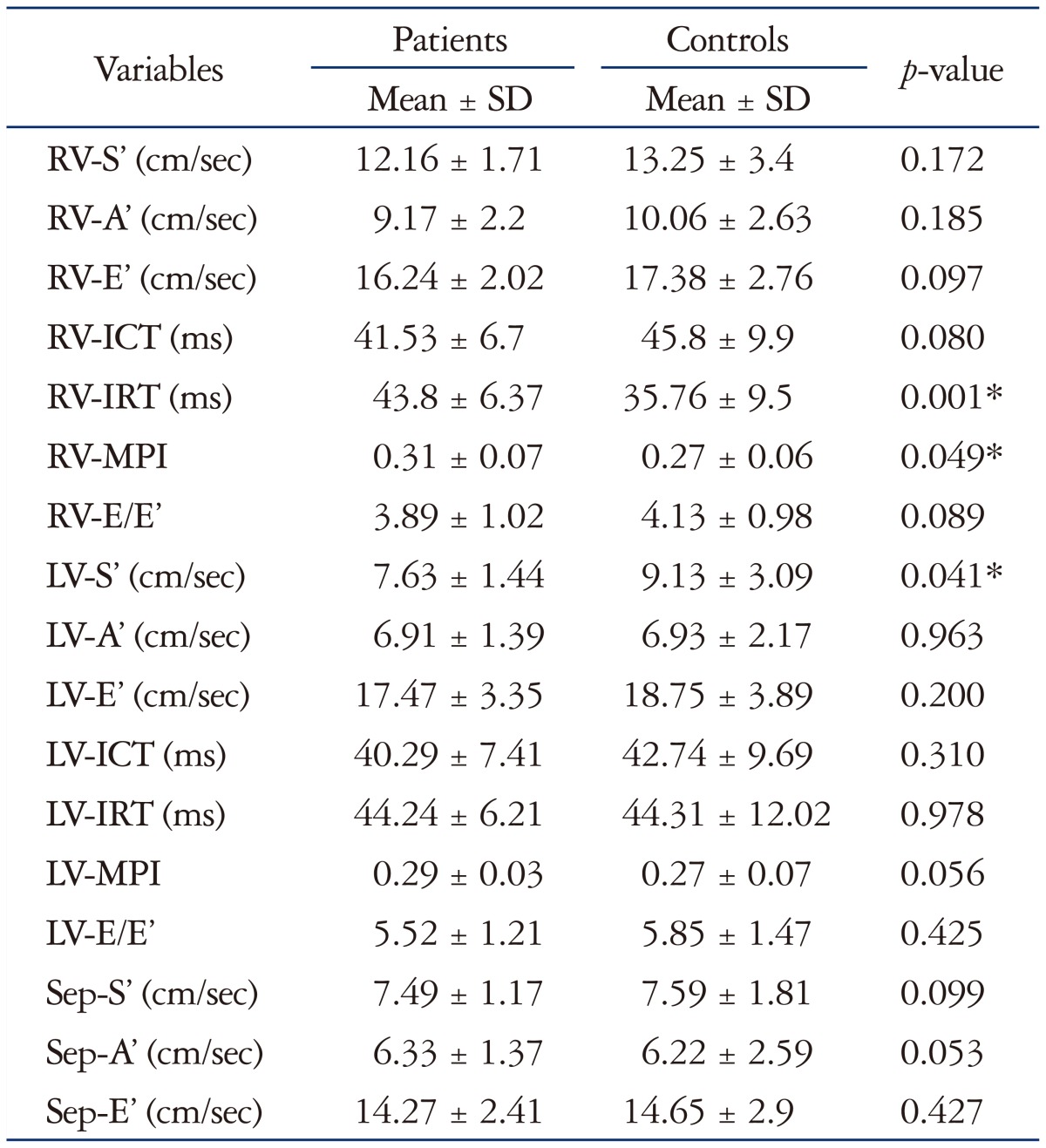
Table 4 shows the comparison between tissue Doppler echocardiographic data of patients and controls. The patients had lower S′ velocity of the RV and LV, shorter IVCT, longer IVRT and lower E/E′ of the RV than controls (p value 0.002, 0.001, 0.004, 0.003, and 0.016, respectively). The MPI of the LV of the patients was significantly higher than controls (p value 0.02).
Good glycemic control was achieved in 12 patients with HbA1c less than 7.5% while the rest of the patients had poor glycemic control. According to the patients' lipid profile, they were grouped into two groups; 13 patients with dyslipidemia and 27 patients without dyslipidemia. Table 5 shows comparison between the M-mode and Doppler findings of patients with good and poor glycemic controls and patients with and without dyslipidemia. Patients with dyslipidemia had significantly higher A wave velocity of the mitral valve (p value 0.047). Table 6 shows comparison between tissue Doppler findings of patients with good and poor glycemic controls and patients with and without dyslipidemia. Patients with dyslipidemia had lower A′ velocity of the LV (p value 0.015).
No significant correlation was found between the duration of diabetes, level of HbA1c or the lipid profile of the patients and the echocardiographic parameters.
Discussion
DCM is defined as the cardiovascular damage present in diabetes patients, which is characterized by myocardial dilatation and hypertrophy, as well as a decrease in the systolic and diastolic function of the LV, and its presence is independent of the coexistence of ischemic heart disease or hypertension.17)
DD refers to abnormalities in ventricular relaxation and filling (RV, LV, or both) with prolonged or incomplete return to presystolic length and force.18) Doppler echocardiography revealed that our patients had significantly lower mitral and tricuspid E and A wave velocities while the E′ and A′ velocities measured by TDI were not reduced in comparison to the controls. On the other hand, the S′ velocities of both LV and RV were significantly reduced in comparison to the controls. The mitral annular or basal LV velocities reflect the long-axis motion of the ventricle, which is an important component of LV systolic and diastolic function. The peak systolic velocity is also a sensitive marker of mildly impaired LV systolic function, even in those with a normal LV ejection fraction or apparently preserved LV systolic function, such as “diastolic heart failure” or in diabetic subjects without overt heart disease.19) Subclinical LV dysfunction may be identified by reduced longitudinal contraction. The radial contractility appears to compensate for reduced longitudinal contractility in subclinical LV dysfunction occurring in the absence of ischaemia or LV hypertrophy.20) Our patients added more evidence on DD in those patients. Other findings which support the presence of subtle DD were longer IVRT, lower E/E′ of the RV and higher MPI of the LV. It is important to emphasize that the DD was more prominent in the RV parameters. These changes reflect early changes in myocardial relaxation. DD in diabetic children was reported by other investigators.21)22)23) LV DD in patients with diabets mellitus (DM) may be caused by increased LV diastolic stiffness, deposition of advanced glycation end (AGE) products, and cardiac fibrosis, all as a consequence of DM.3) This is most likely because of the accumulation of AGE products in the myocardium.24) Accumulation of AGE in collagen was associated with reduced collagen turnover, indicating the possibility that cross-linking of collagen makes collagen resistant to hydrolytic turnover. Such AGE-mediated cross-linking of collagen is thought to be responsible for increased stiffness of arteries and the myocardium.25) The early stages of DCM are dominated by the pathological alterations in the myocardial interstitium, i.e., formation of nonenzymatic (AGEs), impaired compliance, and ischemia from the disease in the vasa vasorum. The morphology of the myocardial cells and small coronary vessels is anatomically preserved. These alterations lead to impaired myocardial contractility. As the disease progresses, LV hypertrophy appears as a result of the hypertrophy of the myocardial cells, the interstitial and perivascular fibrosis, the greater thickening of the capillary basement membrane, and the formation of microaneurysms in small capillary vessels.18) So, more aggressive control of blood glucose levels should be started as early as possible. These results support the concept of a subclinical specific DCM, which develops before obvious systolic dysfunction in patients with T1D mellitus. Existence of a distinct DCM has been claimed to cause DD formerly. In addition, DD has been shown to precede systolic dysfunction in diabetics, even before the presence of pathological findings on clinical examination.26) The natural history of DCM consists of a latent subclinical period, during which cellular structural insults and abnormalities occur initially leading to DD and progressing to degenerative changes, which the myocardium is unable to repair, with subsequent irreversible pathological remodeling. 27) Addition of TDI to posterior wall Doppler has been reported to improve the echocardiographic diagnosis of diastolic impairment in diabetic population. But, unfortunately pediatric DD may not follow the progression seen in adult patients which raise the importance of development of new criteria for children. The pediatric reference data for echo parameters to assess diastolic function successfully define normal controls, but because of the large range of normal values classification of DD maybe difficult.28) Moreover, the recent update for the recommendations for evaluation of LV DD clearly stated that LV DD is present if more than half of the available parameters meet the cutoff values.29)
M-mode echocardiography showed a tendency to ventricular hypertrophy in the absence of hypertension. Our young patients had significantly larger LVIDd and LVIDs diameters and increased IVS and LVPW thickness than controls, but their Z-scores for these dimensions were still within normal for these patients. The LA diameter was also significantly higher in our patients most probably secondary to LV DD. Other investigators reported similar findings.4)26) The FS of LV was significantly lower in our young diabetic patients yet remained within normal values which may imply an early affection of the systolic function. This finding was reported by the Strong Heart Study,30) but their population was different than ours, as they included type 2 diabetes and their patients were much older than ours.
No significant correlation between duration of diabetes and the echocardiographic parameters used to assess the systolic or diastolic function despite that all our patients were diabetic for more than 5 years. Other investigators reported a strong correlation between impairment of diastolic function and DM duration which emphasize the progressive nature of the process, 3)26)31) but the our patients were younger than the patients included in those studies which can explain the discrepancy.
We did not find any correlation between HbA1c and LV or RV diastolic functions this issue may be partly explained by the fact that a single HbA1c may not reflect the overall control of diabetes; in addition, it may cause insufficient and deceptive information about long-term glycemic control. So, the mean HbA1c value averaged over several years instead of a single instantaneous value may provide more accurate information about glycemic control. The influence of HbA1c and diabetes duration was not evident in our study. This relation remains controversial in many studies.
Dyslipidemia in diabetics is a disorder of lipoprotein metabolism that results in increased TC, high LDL, low HDL and high TG. Although dyslipidemia is an established risk factor for cardiovascular disease in T1D adults, no long term studies link between dyslipidemia in T1D children with subsequent cardiovascular disease.32) But lipid abnormality has been linked to the development and prognosis of micro and macrovascular complications in adolescents with T1D.33) Thirteen of our patient had dyslipidemia and they had significantly higher mitral A velocity and lower LV-A′ velocity patients without dyslipidemia. The effect of dyslipidemia is duration dependent. 34) We believe that these findings are possibly a random occurrence of differences because of the large number of variables analyzed. No enough studies regarding effect of dyslipidemia on cardiac function in diabetic children were done.
One of the limitations of this study was that our patients were not subjected to the exercise stress as part of their evaluation which could have yielded more significant results. Another limitation was the use of single HbA1c reading instead of using a mean of readings over several months.
In conclusion, diabetic children have echocardiographic evidence of subtle RV and LV dysfunction with delayed myocardial relaxation. TDI has an additional value in evaluating ventricular filling. This highlights the importance of periodic cardiac evaluation with both conventional and tissue Doppler echocardiography for early detection of this dysfunction.
 XML Download
XML Download