

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cardiac tumors are rare and their incidence among the general population reportedly ranges from 0.001% to 0.03%.1) Over 70% tumors are benign, and atrial myxoma is the most frequent benign cardiac tumor, with an estimated incidence of 0.5 per million individuals per year.2) Most myxomas occur in the left atrium and rarely occur in other sites of the heart. They are sporadic and seldom relapse after complete resection, except the rare Carney complex,3) which is characterized by a combination of multiple myxomas, endocrine hyperfunction, and spotty pigmentation of the skin.4) Additionally, in cases in which multiple cardiac tumors are detected, the tumors are generally malignant or metastatic. Most malignant cardiac tumors are sarcomas, such as angiosarcoma, rhabdomyosarcoma, fibrosarcoma, and leiomyosarcoma. Such tumors can occur in any chamber of the heart, and their prognosis with both surgery and medical treatment is poor. Multiple cardiac tumors are also found in patients with cardiac metastasis. However, little is known about multiple primary myxomas except those that occur as part of the Carney complex. Here, we report a rare case of multiple cardiac tumors that were diagnosed as primary myxomas.
Case
A 78-year-old asymptomatic woman was referred to our hospital for further examination of multiple cardiac tumors in the left atrium and left ventricle, which had been detected on echocardiography conducted before chemotherapy for the third recurrence of breast cancer.
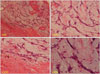
The patient was initially diagnosed with right breast cancer in 2003. She had undergone total mastectomy and lymph node dissection before adjuvant chemotherapy. Histopathological analysis indicated scirrhous carcinoma. The first recurrence of the breast cancer was diagnosed in 2007 due to right axillary adenopathy. She had again undergone operation before receiving chemoradiation, and hormonal therapy was started. The second recurrence was detected in 2013, when computed tomography (CT) was performed during a routine outpatient visit. The CT scan revealed right-sided pleural effusion and a mass shadow in the sternum. After switching to another hormonal medication, the pleural effusion disappeared. The third recurrence was confirmed by skin biopsy of a rash on the postoperative scar. Therefore, the regimen was changed to treat the third recurrence of breast cancer. Adriamycin was selected for the patient, and echocardiography was performed for cardiac screening. There were no signs or symptoms such as fever, shortness of breath, platypnea, and systemic embolization until cardiac tumors were accidentally detected on echocardiography. She had never undergone echocardiography previously. She had no family history of cardiac myxoma. Physical examination and laboratory tests showed no spotty skin pigmentation or endocrine hyperfunction. Transthoracic and transesophageal echocardiograms showed 4 tumors in the left atrium and left ventricle (Fig. 1 and 2). Coronary angiography showed feeding arteries from the left circumflex coronary artery to the tumors and no obstructive coronary lesion. Although we were not confident about the diagnosis, we decided on surgical resection because the mobile tumors located in the left semilunar cusp of the aortic valve and anterior mitral leaflet carried the risk of causing embolism or obstruction. On pathological examination, all 4 tumors were identified as myxomas (Fig. 3), since they showed myxoma cells with a stellate appearance proliferate in a myxoid background in nests and linear syncytia (Fig. 4). The patient's postoperative course was uneventful with no recurrences as determine by echocardiographic examination during the 12-month postoperative follow-up.
Discussion
We identified 2 important clinical issues through the present case study: first, multiple cardiac myxomas can occur in multiple sites of the heart, even in patients without the Carney complex. Second, careful examination is needed to confirm the diagnosis and to determine the best treatment for patients with multiple cardiac tumors.
Cardiac myxoma is usually solitary and sporadic and seldom relapses after complete resection, and in most cases, the lesion is located in the left atrium. In general, multiple cardiac myxomas are characteristic of the Carney complex, which is a dominantly inherited disease in which patients have multiple myxomas, endocrinopathy, and spotty skin pigmentation. The present case did not meet the diagnostic criteria of the Carney complex because the patient had no family history of this condition and no signs of endocrine hyperfunction or skin pigmentation. We first thought that the multiple tumors were metastases, because the patient had a past surgical history and two recurrences of breast cancer. However, postoperative pathological examination of all 4 cardiac tumors showed that they were myxomas, while the primary breast cancer was scirrhous carcinoma. Therefore, we concluded that although multiple cardiac tumors were found in this case, it was not one of the Carney complex, malignant tumors, or metastases.
Non-invasive imaging modalities such as CT, MRI, and 18F-fluorodeoxy glucose positron emission tomography/CT (18F-FDG PET/CT) (PET) may be useful to confirm the diagnosis of multiple cardiac tumors. In the present case, preoperative echocardiography showed mobile tumors in the anterior mitral leaflet and left leaflet of the aortic valve that seemed like they could easily leave the valve. It was difficult to preoperatively diagnose these multiple tumors as myxomas, and we decided on resection because of the risk of embolism and valve obstruction. However, an evaluation using 18F-FDG PET/CT (PET) is indicated, if possible, before the operation. A previous study revealed that 18F-FDG PET/CT (PET) was useful for differentiating malignant and benign cardiac tumors, and the maximum standard uptake value was significantly lower for benign tumors than for malignant primary and secondary cardiac tumors.5)
Detailed evaluation is helpful to determine the best treatment for patients with multiple cardiac tumors. In the present case, the best treatment was surgical resection, because following the resection, multiple cardiac tumors were finally diagnosed as myxoma, for which the long-term prognosis after resection is considerably better than that for malignant metastatic cardiac tumors.
Open heart surgery requiring extracorporeal circulation in cancer patients is another issue highlighted in this case. Heart diseases and cancer are frequently found in Japan, and can coexist in a patient. Open heart surgery with extracorporeal circulation is known to cause transient immunosuppression, which promotes the spread of co-existing cancer cells especially in patients with melanoma and lung cancer.6)7)8) However, some previous studies found no significant difference in survival rates between cancer patients and individuals from the normal population undergoing open heart surgery.9)10) Through our experience in this case, we emphasize the importance of careful examination to confirm diagnosis and the importance of individual evaluation to determine the best treatment, because multiple myxomas can occur in multiple sites of the heart, and open heart surgery may not be harmful even in cancer patients.



 XML Download
XML Download