

 PDF
PDF ePub
ePub Citation
Citation Print
Print


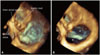
A 75-year-old man with atrial fibrillation was hospitalized because of shortness of breath triggered by upper respiratory infection and tachycardia. His symptoms were improved by bed rest and administration of diuretics. Pretreatment echocardiogram reported dilatation of the right ventricle (RV). Follow-up study was performed before discharge. Apical four-chamber view still demonstrated remarkable dilatation of RV (Fig. 1A). In one of the apical four-chamber views, the tricuspid valve showed a bridge-like appearance in systole without valve opening (Fig. 1B and C, Supplementary movie 1). The RV inflow view (Fig. 1D, E, and F, Supplementary movie 2) revealed localized small leaflet defect at posterior septum (Fig. 1D) with the opposing leaflet tip coapting against the RV wall (Fig. 1D). At the anterior side of the "bridge", another valve orifice was observed in RV inflow view as well as parasternal short-axis views (Fig. 1G, H, and I, Supplementary movie 3). Color Doppler images in these views showed flow from the RV to right atrium across two orifices (Fig. 1F and I), suggesting double-orifice tricuspid valve.1)2) There was no pressure gradient across both orifices in diastole. Tricuspid regurgitation jet velocity of less than 3 m/s was observed from both orifices in systole. Three-dimensional transthoracic echocardiography clearly visualized double orifices (Fig. 2, Supplementary movie 4) and confirmed the diagnosis.
Figures and Tables
Fig. 1
Transthoracic echocardiographic views of the tricuspid valve in the apical four-chamber (A, B, and C), right ventricular inflow (D, E, and F), and parasternal basal short-axis (G, H, and I) views shown without (first 2 columns) and with color Doppler (last column). The tricuspid valve has a bridge-like appearance (B, white arrows) in the apical four-chamber view. A defect is seen at the posterior septum (D, white arrow) and the leaflet tip coapts against the right ventricular wall (D, yellow arrow). The double orifice can be appreciated in the right ventricular inflow view (E and F) and the basal short-axis view (H and I).

Supplementary movie legends
Movie 1
Two-dimensional apical four-chamber view showing the behavior of the tricuspid valve throughout the cardiac cycle. The coaptation point is not seen on this clip.
Movie 2
Two-dimensional right ventricular inflow view showing the tricuspid valve. Two orifices can be appreciated.
 XML Download
XML Download