

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Patients with pulmonary arterial hypertension (PAH) have a high mortality rate despite earlier disease recognition and availability of new drug treatments which have improved survival in recent years.1)2)3) Irrespective of the etiology of PAH, right ventricular (RV) function is the main determinant of symptoms and survival.4)5) Because transthoracic 2-dimensional echocardiography (2DE) gives us important information about cardiac structures, RV function and hemodynamic status, it is one of the most commonly used modalities for screening and monitoring of the effect of medical management. However, the complex shape of the RV chamber makes accurate assessment by conventional 2DE imaging difficult.6) Moreover, conventional velocity and displacement based analyses can be affected by translational motion of the heart and respiratory variation.7) New 2-dimensional strain echocardiography enables quantification of both regional and global myocardial function in a simple and angle-independent manner.8) Although 2-dimensional strain echocardiography was introduced to evaluate global left ventricular (LV) function, it has recently been used to assess RV function.9)10)
Global longitudinal strain of RV (GLSRV) can be measured with 2-dimensional strain analysis and thus can give a more direct assessment of RV mechanics. In patients with PAH, decreased RV strain was associated with poor prognosis in the previous study.11) Because RV has different anatomy and function compared with LV, the simple application of strain algorithm to RV remains problematic. Also, there are several vender-different algorithms in the measurement of strain. Velocity vector imaging software (VVI; Axius, Siemens Medical Solutions, Mountain View, CA, USA) can measure RV strain without an influence of ventricular wall thickness. So, we measured GLSRV in patients with PAH with VVI and evaluated its prognostic significance.
Methods
Study population
We studied consecutive adult patients (age more than 18 years old) with PAH evaluated from February 2007 to June 2008 in the PAH clinic of Cleveland Clinic. All patients fulfilled the contemporary diagnostic criteria by the Third World Symposium of PAH and they had regular outpatient follow-ups.12) Patients with LV systolic dysfunction, significant valvular heart disease, chronic thromboembolic disease and pulmonary parenchymal diseases were excluded in this study. We analyzed total 51 patients with PAH [34 idiopathic, 13 familial, and 4 associated with other diseases (2 with connective tissue disease, 1 with myeloproliferative disease and 1 with systemic to pulmonary shunt)]. This study protocol was approved by the Cleveland Clinic Institutional Review Board.
Echocardiography
Conventional 2DE examinations were performed using a Vivid 7 ultrasound system (GE-Vigmed, Horten, Norway) according to the guidelines and standard recommendations of the American Society of Echocardiography.13) All echocardiographic images were digitally stored and were reviewed by sonographers (J.-H.P. and M.P.) unaware of the clinical, laboratory, and hemodynamic information. Conventional echocardiographic parameters were measured by an investigator (M.P.) and reviewed by an investigator (J.T.). RV fractional area change (RVFAC) was calculated from the apical 4-chamber view using the percentage change in areas of the end-diastolic and endsystolic areas of the RV. The tricuspid annular plane systolic excursion (TAPSE) was recorded with M-mode echocardiography parallel to the lateral RV wall and across the tricuspid annular plane and measured as the distance of systolic movement of the RV annulus in the longitudinal direction.6) RV myocardial performance (Tei) index was defined as the ratio of isovolumic relaxation time and isovolumic contraction time divided by ejection time of RV.6)
Pulmonary artery systolic pressure was estimated from the maximal continuous-wave Doppler velocity of the tricuspid regurgitation (TR) jet imaged from multiple planes plus estimated central venous pressure calculated by the diameter of inferior vena cava and distensibility.6) An index of pulmonary vascular resistance was derived by dividing the maximal velocity of the TR jet by the RV outflow tract velocity-time integral.14) An average of 3 measurements was used for all analyses.
RV strain and strain rate were analyzed off-line with VVI by another investigator (J.-H.P.). After manual tracing of the endocardial border of the RV (about 10 to 16 points) over one frame, the endocardial borders were automatically tracked throughout the cardiac cycle. The measurement of RV longitudinal strain by VVI showed relatively good correlation with cardiac magnetic resonance data.15) Myocardial velocity is derived as the ratio between frame-to-frame displacement of the speckles and the time interval.8) Systolic longitudinal strain, time-to peak strain, and peak systolic and diastolic strain rate were calculated. Negative strain values indicate tissue shortening and a smaller value (that is, higher absolute value) indicates better RV systolic function. GLSRV was calculated by the average of six segmental values. Longitudinal strain of RV free wall and interventricular septum were measured by the averages of three segmental values (base, mid, and apex) of the lateral wall and interventricular septum. Because strain expresses deformation relative to the initial length, systolic shortening in the longitudinal orientation is expressed in negative numbers. Lower GLSRV value means better RV systolic function.
Clinical outcomes
Patients were followed over 45 ± 15 months for a composite of death, cardiac hospitalization due to worsening of heart failure and lung transplantation. The presence of adverse clinical events was determined with reviewing their medical records in patients with regular clinical follow-ups. In patients without clinical follow-up, the presence of death was checked with medical records or the Social Security Death Index.
Statistical analysis
The data were analyzed using standard software (SPSS version 20.0, IBM Co., Chicago, IL, USA). Summary data were expressed as mean ± standard deviation or percentage of patients. Linear regression analysis was performed to evaluate the relationship between GLSRV and other variables. The optimal cutoff value of GLSRV for predicting adverse clinical events was determined by the receiver-operating characteristic curve analysis. Reclassification was evaluated with net reclassification improvement (NRI) methods described by Pencina et al.16) NRI measures the improvement in response using event-specific reclassification tables. Cox proportional hazard model with bootstrapping was used to assess the association of variables with end points. Hazard ratios (HR) are given with their 95% confidence intervals (CI) and the HR refers to a unit increase in the variables. Variable selection in multivariate analysis was based on statistical significance at univariate analysis. To avoid multicollinearity, redundant echocardiographic variables were dropped from the multivariate regression model in the case of pairwise correlations between continuous variables exceeding 0.50 as Pearson's correlation coefficient, including the variable with the strongest individual effect size.17) The event-free curves were based on Kaplan-Meier analyses stratified by GLSRV value and the comparisons were made by Log-rank test.
Intraobserver and interobserver variabilities of the GLSRV were evaluated in 15 random subjects by two investigators (J.-H.P. and M.P.), and measured by calculating the intraclass correlation coefficient (ICC), coefficient of variance (COV) and limits of agreement. A p value less than 0.05 was considered statistically significant.
Results
Patient characteristics
A total 51 patients (40 females mean age 48 ± 14 years old) were included in this study. Their mean duration of disease was 46 ± 35 months and the majority of patients were World Health Organization functional class II (61%) and III (35%). Twenty two patients were taking a single vasodilator medication [2 on calcium channel blocker (CCB), 5 a phosphodiesterase-5 inhibitor (PDE5I), 3 an oral endothelin receptor antagonists (ERA), and 12 prostaglandins] and 29 patients were taking a combination of vasodilators (2 on CCB and PDE5I, 1 on CCB and ERA, 6 on PDE5I and ERA, 7 on ERA and prostaglandins, 5 on PDE5 and prostaglandins, and 8 on PDE5I, ERA and prostaglandins). Twenty eight patients received oral diuretic therapy to reduce their peripheral edema and 28 were anticoagulated with oral warfarin. The baseline clinical, laboratory, conventional echocardiographic, and right heart catheterization data (Table 1) are typical for a PAH population, with normal LV systolic function, elevated pulmonary arterial pressure, RV enlargement and RV dysfunction.
RV strain findings
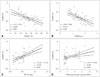
Global and regional two-dimensional strain measurements are listed in Table 2. GLSRV and systolic strain rate of RV were significantly decreased than normal RV strain values in the previously reported paper.6) The average GLSRV was -16.1 ± 5.0% and average systolic strain rate of RV was -1.28 ± 0.38 s-1. GLSRV showed a good negative correlation with RVFAC, TAPSE and RV Tei index. GLSRV demonstrated a significant correlation with pulmonary vascular resistance (PVR) calculated by right heart catheterization (Fig. 1). RV free wall strain also revealed significant correlations with RVFAC (r = -0.629, p < 0.001), TAPSE (r = -0.551, p < 0.001), RV Tei index (r = 0.607, p < 0.001) and PVR (r = 0.495, p < 0.001).
Follow-up
During the follow-up of 45 ± 15 months, 20 patients had experienced one or more adverse events including 12 deaths, 2 lung transplantation and 15 hospital admissions due to worsening heart failure. After univariate analysis, adverse clinical events were associated with age, 6-minute walking distance (6-MWD), B-type natriuretic peptide (BNP) concentration, right atrial size, TAPSE, RVFAC, and GLSRV. In the prediction of mortality, age, 6MWD, BNP concentration, and GLSRV were statistically significant variables after univariate analysis (Table 3). After multivariate analysis, age and GLSRV remains statistically significant in the prediction of adverse clinical events and mortality (Table 4). The best cutoff value of GLSRV for detection of adverse clinical events was -15.5% (95% CI = -16.9 -10.9%) with a sensitivity of 70% and specificity 77%. The value (GLSRV ≥ -15.5%) offered an improvement in reclassification of prediction of adverse clinical event or death by TAPSE (< 1.5 cm) or the presence of pericardial effusion (Table 5). PAH patients with impaired GLSRV (≥ -15.5%) showed lower eventfree survival (80 ± 7% vs. 42 ± 11% at 4 years, p < 0.001) and lower total survival (93 ± 5% vs. 57 ± 11% at 4 years, p < 0.001) than preserved GLSRV patients (Fig. 2).
Variability
Intraobserver variability: ICC was 0.950 (95% CI = 0.854-0.983, p < 0.001), COV was 9.7% (95% CI = 3.4-14.1%), and 95% limits of agreement was -3.5 to 4.5%.
Interobserver variability: ICC was 0.918 (95% CI = 0.757-0.973, p < 0.001), COV was 12.9% (95% CI = 5.1-18.8%), and 95% limits of agreement was -5.5 to 5.2%.
Discussion
The main findings of this study are that GLSRV is a readily obtained echocardiographic parameter, which correlates well with other conventional indices of RV systolic function on routine transthoracic echocardiographic examination. Furthermore, worse GLSRV (≥ -15.5%) independently predicts adverse clinical events and death in patients with PAH.
Although imaging quality has improved, assessment of the diseased RV by conventional 2DE standards remains a difficult issue. The complex shape and different systolic mechanics of the RV chamber are possible explanations.6) Delineation of the endocardial border in the measurement of RVFAC may limit the reliability in assessing RV function. Tethering and translational motion can affect the use of velocity and displacement based measurements like TAPSE.10)
Speckle tracking has been introduced for the assessment of the LV function. The use of speckle tracking for the assessment of regional and global LV function has been validated by sonomicrometry,18)19) and it enables the measurement of the ventricle non-geometrically. Strain has an advantage over velocity and displacement based measurements as being relatively independent of tethering or translational motion.10) Myocardial strain can be used to detect early stages of myocardial dysfunction and it has prognostic power in patients with chronic heart failure.20)21)22) Though strain is initially developed to measure LV mechanics, speckle strain has been utilized for the assessment of the RV in some disease categories.8)10)23) Because RV has thinner free wall thickness than LV, simple application of strain algorithm to RV remains problematic. We applied strain to RV including RV free wall and interventricular septum together. In the previous study of the comparison of RV longitudinal strain with RV ejection fraction (RVEF) calculated by cardiac magnetic resonance imaging (CMR), global RV longitudinal strain including RV free wall and interventricular septum showed more better correlation with RVEF by CMR.24) Our current study showed that the mean GLSRV of the patients with PAH was -16.1%. These absolute values are considerably lower than those of normal subjects (normal mean value of global longitudinal strain of RV by 2-dimensional echocardiography is about -28%).6) In PAH patients, chronic pressure and volume overload of RV leads to both structural and functional changes.1)25) Puwanant et al.23) reported longitudinal deformation of RV free wall in patients with chronic PAH is significantly decreased compared with control subjects.
Lower GLSRV (≥ -15.5%) was associated with adverse clinical event and death in our study. Moreover, GLSRV ≥ -15.5% offered an improvement in reclassification of prediction of adverse clinical event or death by TAPSE (< 1.5 cm) or the presence of pericardial effusion which are known as bad prognostic factors in PAH patients. This finding correlates with the previous reports by other investigators.23)26) In contrast from these aforementioned studies, we used a global longitudinal strain value of the RV which included the interventricular septum. In the strain assessment of the RV, long-axis assessment is performed in the RV free wall only or the RV free wall with interventricular septum together. Because the interventricular septum has both RV and LV mechanical components, its strain assessment can be complicated. However, chronic pressure overload of the RV can affect ventricular geometry and the interventricular septum also plays an important role in the systolic RV mechanics.23)27) We included the interventricular septum in our overall global RV strain assessment to precisely evaluate RV systolic function by strain analysis. In our study, RV free wall strain showed similar significant correlations with conventional echocardiographic RV parameters. However, using global RV strain including septum [area under the curve (AUC) = 0.734, 95% CI = 0.592-0.848] has larger AUC than that of RV free strain (AUC = 0.677, 95% CI = 0.532-0.801) in the prediction of adverse clinical events (difference = 0.06, p = 0.0448) after comparison of AUC's with the method suggested by Hanley and McNeil.28)
This study has several limitations. First, this is a retrospective cohort study with a variety of disease causes and concurrent PAH therapy, which may have affected the pulmonary arterial systolic pressure and subsequent RV loading conditions. Second, there was no reference study like cardiac magnetic resonance imaging in the measurement of RV systolic function objectively. A prospective study with a large number of patients with an objective comparison method will be needed to confirm the correlations and the clinical impact of this measurement.
Future directions
With RV strain validated as an important prognostic variability in PAH patients, it will be critical to test whether it can serve as a surrogate endpoint for novel therapies in PAH. If improvement in GLSRV with vasodilator or other intervention identifies those with better clinical outcomes, then drug development in PAH could be accelerated.
In conclusion, GLSRV showed significant correlations with conventional echocardiographic parameters of the RV systolic function. Lower absolute GLSRV is associated with the presence of adverse clinical events and deaths in patients with PAH.






 XML Download
XML Download