

 PDF
PDF ePub
ePub Citation
Citation Print
Print


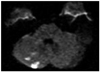
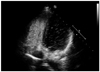
A 31-year-old woman referred to evaluate the cause of sudden dizziness. She had no history of diabetes, hypertension, arrhythmias or stroke. Auscultation showed clear lung sound and no cardiac murmurs. Chest radiography and electrocardiogram did not show any abnormalities. Laboratory tests for hypercoagulability and vasculitis were all negative. In the previous hospital, she took brain magnetic resonance imaging, which revealed newly developed multiple right cerebellar infarction (Fig. 1). Transthoracic echocardiography and transesophageal echocardiography (TEE) for the evaluation of embolic source showed the right-to-left shunt, but the cause of shunt was inconclusive. After transfer, we repeated contrast echocardiography using agitated saline and reaffirmed a delayed appearance of a substantial amount of microbubbles in the left atrium (Fig. 2). However, we could not depict a passage of microbubbles through the gap between interatrial septum to confirm the presence of patent foramen ovale (PFO). Thus, we evaluated all the pulmonary veins, one by one during TEE and finally revealed the microbubbles in a row coming from the left lower pulmonary vein (Fig. 3 and Supplementary movie 1). These findings suggested the presence of a pulmonary arterio-venous fistula (PAVF) in the left lower pulmonary lobe, possibly causing paradoxical embolisms. The diagnosis was confirmed by a computed tomography pulmonary angiography which revealed the fistula located posteriorly in the left lower pulmonary lobe (Fig. 4, arrow). After successful occlusion of the fistula, the patient was discharged with warfarin.
Both PFO and PAVF could contribute to the development of right-to-left shunt.1) Presence of PAVF and the draining pulmonary vein could be accurately identified by TEE. We need to routinely examine the presence of PAVF during TEE in the evaluation of embolic source.


 XML Download
XML Download