

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Prosthetic valve thrombosis (PVT) is one of the most serious complications of prosthetic heart valves. The overall incidence is reported to range from 0.1% to 5.7% per patient year.1) The incidence of PVT is differed from the valve position, it reported as 0.5% per patient-year in the mitral position2) and 1% to 4% in the tricuspid position.3)4) Although the incidence of PVT of tricuspid position is high, there are not enough data on the management of it, in contrast to left-sided PVT.5-8) Also identifying a thrombus on a tricuspid prosthesis with transthoracic echocardiography (TTE) or trans-esophageal echocardiography (TEE) is more challenging than mitral prosthesis, especially if the thrombus is non-obstructive. We herein present a case of tricuspid PVT which was diagnosed with multi-detector-row computed tomography (MDCT) and successfully treated without thrombolytic therapy or surgery.
Go to : 
Case
A 57-year-old female patient was admitted to the hospital with the complaint of dyspnea [The New York Heart Association (NYHA) Functional class II] in December, 2010. TTE showed left ventricular ejection fraction of 59%, severe mitral stenosis, severe aortic stenosis and severe tricuspid regurgitation. In January 2011, the patient underwent mitral valve replacement with a 25 mm On-X Valve (On-X Life Technologies Inc., Austin, TX, USA), tricuspid valve replacement with a 31/33 mm On-X Valve, and aortic valve commissurotomy. Also, because of persistent atrial fibrillation, she received Cox-maze procedure. Eleven days after valve replacement, TTE revealed that the normal function and gradients of the two prosthetic valves. At the time of discharge, the patient's international normalized ratio (INR) was 2.36. She was discharged from the hospital with the recommendation to use warfarin with goal INR 2.0-3.0.
In December 2012, the patient complained of dyspnea again. Her blood pressure was 137/68 mmHg and pulse rate was 55 beats per minute. TTE and TEE demonstrated that two prosthetic valves had normal functions and gradients. Doppler echocardiographic examination of the prosthetic tricuspid valve demonstrated the peak E velocity of 1 m/s, peak pressure gradient of 5 mmHg, and pressure half time of 144 ms (Fig. 1). Fluoroscopic evaluation revealed that both leaflets of the two prosthetic valves moved freely. She complained of intermittent, small amount of melena and microcytic and hypochromic anemia with hemoglobin level of 7.8 mg/dL was detected. Therefore, under impression of iron deficiency anemia caused by gastrointestinal bleeding, oral iron supplement was prescribed and esophagogastroduodenoscopy (EGD) was planned. The patient's INR was 2.51 before procedure. After four days of withholding warfarin therapy without reversal the effect of it, EGD was done. Her INR was 1.82 at that time. EGD showed erosive gastritis without active bleeding focus, no hemostatic intervention was performed and the patient resumed taking warfarin the next day.
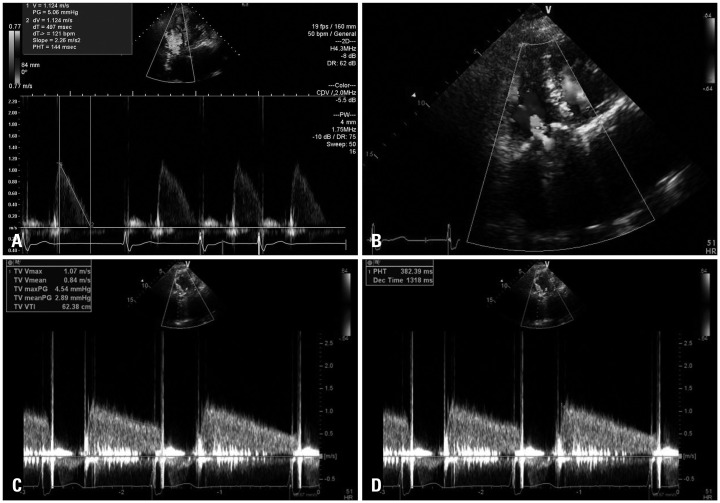 | Fig. 1A: Doppler echocardiographic examination before warfarin discontinuation shows the peak E velocity of 1 m/s, peak pressure gradient of 5 mmHg, and normal range of pressure half time of 144 ms. B-D: Transthoracic echocardiography at admission. (B) Doppler echocardiography shows a mosaic pattern of the color Doppler signal at the tricuspid inflow. (C) Continuous Doppler examination demonstrates the mean and peak pressure gradient of 3 mmHg and 5 mmHg (D), and an increased pressure half time of 382 ms across the tricuspid valve.
|
The patient was hospitalized for evaluation of the causes of worsening dyspnea (NYHA Functional class III) despite correction of anemia in February 2013. On admission day, her blood pressure was 121/59 mmHg, pulse rate was 80 beats per minute and INR was 2.13. TTE revealed that the prosthetic mitral valve had normal function and gradients, whereas the prosthetic tricuspid valve showed limited motion without definite obstruction. Doppler measurements including peak E velocity and mean gradient, however, were within acceptable range. The peak E velocity was 1 m/s and mean gradient was 3 mmHg. The only parameter suggested prosthetic tricuspid valve dysfunction was prolonged pressure half time, 382 ms (Fig. 1). Considering the fact that warfarin was recently discontinued, fluoroscopic evaluation was done. The fluoroscopy showed that one leaflet of the prosthetic tricuspid valve had limited motion (Supplementary movie 1). For evaluation of the cause of impaired prosthetic tricuspid valve motion, MDCT was performed. Computed tomography demonstrated the large thrombus on prosthetic tricuspid valve (Fig. 2, Supplementary movie 2 and 3). With the diagnosis of prosthetic tricuspid valve thrombosis, the patient was administered 60 mg of low molecular weight heparin twice a day for three days. Her blood pressure and pulse rate were stable during hospitalization. After three days, she discharged from the hospital with the recommendation to adjust warfarin dose with goal INR 3.0-3.5. Two weeks after discharge from the hospital, she visited the outpatient clinic for follow-up. Dyspnea was disappeared and her exercise capacity was improved. Then, after four months, follow-up TTE was done. The images showed unrestricted motion of prosthetic tricuspid valve with normal pressure half time (Fig. 3).

Go to :
Discussion
Prosthetic valve thrombosis is a rare, but serious complication. The lower pressures on the right side of the heart with a slower blood flow across the tricuspid valve are the important cause of higher risk of thrombus formation in prosthetic tricuspid valves. Moreover, the risk is even higher in prothrombotic states such as pregnancy or atrial fibrillation, with inadequate anticoagulation, and in patients with multiple prosthetic valves.9) Our patient with atrial fibrillation and multiple prosthetic valves including tricuspid prosthesis had high risk of thromboembolism. The American Society for Gastrointestinal Endoscopy guidelines recommend that warfarin should be discontinued for 3-5 days in high-risk patients undergoing high risk procedures, and consideration should be given to bridging therapy with heparin or low molecular weight heparin.10) However, these provide limited guidance only with elective situations and there are few recommendations during the acute gastrointestinal hemorrhage and care after the procedures. Although the previous studies showed low incidence of thromboembolic events with warfarin withhold,11)12) in light of high risk of thromboembolism, bridging therapy with heparin might be needed to prevent thrombotic complication in our patient.
The diagnosis of PVT is usually confirmed by TTE, TEE and cine-fluoroscopy. TTE is often the first modality of diagnostic assessment. However, acoustic shadowing and artifacts created by the mechanical prosthetic valves limit the availability of TTE to evaluate the motion of the leaflets. Also, in non-obstructive PVT, TTE is commonly normal. Doppler parameters have been aided to detect prosthetic valve dysfunction. According to the guideline from the American Society of Echocardiography, obstruction of prosthetic tricuspid valve suggested on continuous wave Doppler by an E velocity > 1.7 m/s, mean gradient > 6 mmHg or pressure half-time > 230 ms. In this case, increased pressure half time was the only abnormal parameter.13)14) Suspicion based on history, and thorough echocardiographic examination was the key role in the diagnosis of non-obstructive PVT.
After performance of TTE and cine-fluoroscopy, the diagnosis is usually confirmed by TEE. However, tricuspid valve evaluation via TEE is difficult because of complex structure and relative distance from the esophagus. Therefore, we chose MDCT as a diagnostic tool for the confirmation of PVT. MDCT can provide sharp images to characterize the reduced mobility of prosthetic leaflets or even directly visualize and distinguish between thrombus and pannus.15-17) In the present case, MDCT provided good image quality of prosthetic tricuspid valve and showed large size of thrombus directly.
Once diagnosis of PVT is confirmed, several therapeutic modalities can be considered: surgery, fibrinolysis, heparin treatment, or optimization of anticoagulation therapy. Selecting one of these modalities is largely influenced by the presence of valvular obstruction, valve location (left- or right-sided), and clinical status. According to the guidelines of American Heart Association/American College of Cardiology, thrombolytic therapy is reasonable for thrombosed right-sided prosthetic heart valves with NYHA functional class III-IV symptoms or a large clot burden.18) The European Society of Cardiology guideline also recommends thrombolytic therapy for tricuspid PVT.19) However, even the consideration of relative lower complication rates of right-sided PVT, thrombolytic agents are associated with risks of embolism and bleeding. In tricuspid valve thrombosis, Shapira et al.8) reported one patient who has mild symptom treated effectively by intensifying anticoagulation. Even in left-sided PVT, Al Habib et al.20) reported a patient who successfully treated of mechanical mitral valve thrombosis with antithrombotic agents alone. In this regard, in stable patients with non-obstructive, intensification of anticoagulation can be an alternative therapy.
In this case, the patient suffered from exertional dyspnea and TTE showed no significant hemodynamic change except increased pressure half time. Suspicion, thorough echocardiographic examination and MDCT attributed in the diagnosis. Despite large thrombus size, our patient successfully treated by low molecular weight heparin bridging therapy followed by intensifying anticoagulation. Although this conservative approach is inappropriate as first-line therapy, we do suggest that high dose anticoagulation therapy alone could be a reasonable therapeutic option for patients with hemodynamically stable tricuspid PVT.
Go to :

 XML Download
XML Download