

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Myxoma is the most common primary cardiac tumor and has a prevalence of 0.5 cases per million people per year, of which only 2% to 4% arise in the right ventricle.1) Cardiac tumors located in the right ventricular outflow tract (RVOT) are quite rare and present unusual diagnostic and therapeutic challenges. A right-sided cardiac tumor can present with signs and symptoms of right heart failure or RVOT obstruction, and surgical removal is the treatment of choice.
Case
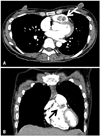
A 42-year-old female presented with general weakness occurring over 3 months. She was a hepatitis B carrier and had undergone prior surgeries for benign breast nodules and a parotid gland tumor. She had also been recently diagnosed with uterine myoma. On admission, she had a normal temperature of 36.5°C, blood pressure of 120/80 mmHg, pulse rate of 100 beats/min, and respiratory rate of 16 breaths/min. There was no history of fever or weight loss. Thoracic auscultation revealed clear lung sounds without crackles and regular heart beat without murmur, but she had pale conjunctiva. Electrocardiogram and chest radiograph were unremarkable. Laboratory data were within normal range for white blood cell count, erythrocyte sediment rate and C-reactive protein level, but there was evidence of microcytic anemia (hemoglobin 6.3 g/dL, mean corpuscular volume of 65.6 fL, serum iron 10 mcg/dL, total iron binding capacity 474 mcg/dL, serum ferritin 1.73 ng/mL). Serologic tests for autoimmune markers were also negative. Although uterine myoma was thought to be the main cause of anemia, abdominal computed tomography (CT) was performed to identify any other possible causes of bleeding, and a large mass in the pulmonary outflow tract was found incidentally. Pulmonary angio CT showed a contrast-enhancing mass in the RVOT (Fig. 1). Transthoracic Doppler echocardiography (TTE) was performed for further evaluation of the RVOT mass and revealed a large, mobile, ovoid mass measuring 24 × 17 mm in diameter, which was prolapsing into the pulmonary trunk during the systolic phase (Fig. 2). Although we were not able to obtain a pulse wave Doppler measurement across the obstruction owing to a non-favorable interception angle, there was no definite flow acceleration around the tumor by color flow Doppler. The right ventricle (RV) chamber was mildly dilated, but there was no significant tricuspid regurgitation or right ventricular hypertrophy, and the estimated RV systolic pressure was 36 mmHg. Transesophageal echocardiography was performed to confirm the size and location of the mass, showing the stalk of the mass originating from the subvalvular infundibulum (Fig. 3).
The patient underwent surgery and the mass was completely removed via right atrial approach under cardiopulmonary bypass (Fig. 4A). The mass was yellowish, soft and had a wide stalk. Microscopic examination showed stellate and globular cells that were arranged in a cord-like pattern with an abundant myxoid background, consistent with a benign myxoma (Fig. 4B). The patient's postoperative course was uneventful and she was discharged 10 days after surgery.
Discussion
Cardiac myxoma is usually seen in adults, but also accounts for 24-40% of all cardiac tumors that occur between birth and adolescence. The majority of myxomas (75%) are located in the left atrium, whereas RV myxoma is only found in 2-4% of cases, and RVOT myxoma is quite rare.2) Only 4 cases of RV myxoma have been reported in Korea; these were located in the RV free wall, the tricuspid valve, the anterior papillary muscle and the interventricular septum, causing significant flow obstruction. 3-6) Right-sided cardiac tumors can present with symptoms and signs of right heart failure or RVOT obstruction, and, particularly in the case of RV myxoma, complications of vena cava syndrome, pulmonary embolism and RV dysfunction have been reported.2) The tumor mass in this case was originated from the RVOT, and no flow acceleration was observed by color Doppler. Although RVOT flow obstruction cannot be excluded completely because of the absence of pulse wave Doppler measurement, this case seems to be unique in that peripheral edema, hepatomegaly, hash systolic murmur by flow obstruction and other incidental findings typical to previously reported cases were absent. Surgical removal is regarded as the gold standard treatment for cardiac myxoma, and various surgical approaches through the right atrium or the right ventricle have been reported. The right atrial approach is effective in most cases of small-to average-sized right ventricular myxoma; the right ventriculotomy approach may cause postoperative right ventricular dysfunction, and is therefore not advisable.7)8) In this case, successful excision was performed through the right atrial approach.
This patient had multiple tumors prior to cardiac myxoma, including breast nodules, a parotid gland tumor, and uterine myoma. However, there was no family history of cardiac tumor and the Carney's complex was absent on examination. Although our patient did not meet the diagnostic criteria for Carney's complex, to the best of our knowledge, cardiac myxoma accompanied by the tumors mentioned above has not been reported previously. Further evaluation with genetic study and serial follow-up may be required to establish any relevant association between the multiple tumors in this patient.
The present case indicates that serial TTE follow-up might be helpful in detecting incidental cardiac tumors, especially in patients with a history of multiple tumors.



 XML Download
XML Download