

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Mitral regurgitation (MR) is commonly found on echocardiography and is usually hemodynamically insignificant. However, severe MR needs immediate attention, especially in patients with organic mitral valve disease with a repairable valve because these patients may benefit from early surgery.1) Although quantitation of all detected MR is ideal, such quantitation is impractical, given the large number of patients with some degree of MR. Therefore, some authors have suggested using mitral E wave velocity and the E wave to A wave ratio (E/A) as the screening tools to rapidly exclude patients without severe MR.2) On the basis of a limited number of studies, American Society of Echocardiography (ASE) guidelines stated that, "In severe MR without stenosis, the mitral E velocity is higher than the velocity during atrial contraction (A velocity) and is usually greater than 1.2 m/sec. A mitral inflow pattern with an A-wave dominance virtually excludes severe MR".3) In addition, the European Association of Echocardiography suggests that "In the absence of mitral stenosis, a peak E wave velocity > 1.5 m/sec suggests severe MR. Conversely, a dominant A wave virtually excludes severe MR".4)
However, the studies evaluating the utility of E wave velocpity have not included many patients with severe MR due to flail mitral valve leaflets and requiring surgery, thereby making the conclusions of the studies less strong.2) In addition to MR, E wave velocity is dependent on several factors, including abnormal relaxation and high left ventricular filling pressures. Not infrequently, patients with severe organic MR due to flail leaflets have lower-than-expected E wave velocity or a dominant A wave pattern, or both, on their mitral inflow in our clinical practice. We hypothesized that the accepted mitral E velocity of 1.2 m/sec has low sensitivity to exclude severe MR and mitral A wave dominance pattern alone cannot exclude severe MR in all patients.
Methods
We retrospectively reviewed medical records of patients aged 18 years and older who underwent a transthoracic echocardiogram and subsequent mitral valve surgery for mitral valve disease at Mayo Clinic in Arizona between 1987 and 2010. We included only those patients with normal left ventricular ejection fraction (EF) who underwent surgery because of quantified severe MR due to either mitral valve prolapse or flail mitral valve leaflet. We excluded patients who did not have a transthoracic echocardiogram within 1 year of surgery; did not undergo surgery; had an EF less than 60%; had greater than mild valvular stenosis or regurgitation in the aortic, pulmonic, or tricuspid valves; were paced due to an implanted pacemaker; were in atrial fibrillation; had poor-quality images; and had any congenital abnormality, including atrial septal defect and hypertrophic obstructive cardiomyopathy.
A total of 35 patients were ultimately selected from 300 patients who eventually met the inclusion and exclusion criteria and constituted the final study group. These patients were compared to 35 age-matched control subjects selected sequentially from patients who underwent echocardiographic study at our institution, were in sinus rhythm, and had either no or only mild valvular regurgitation and a normal left ventricular EF.
Standard comprehensive 2-dimensional Doppler echocardiographic examinations were performed using a commercially available system-Sequoia C512 (Siemens AG, Oceanside, CA, USA) or Vivid 7 (GE Healthcare, Waukesha, WI, USA). The quantification of severe MR was in accordance with the recommendations from the ASE.3)
Briefly, the concept of proximal isovelocity surface area (PISA) is based on flow convergence proximal to the regurgitant orifice.5)6) The blood accelerates as it enters a regurgitant orifice and produces a series of shells. Applying the principle of conservation of mass, the regurgitant flow rate and regurgitant volume can be calculated.7) The following additional standard echocardiographic data were also evaluated in each patient: EF, left ventricular end diastolic and systolic dimensions, E wave velocity, A wave velocity, tissue Doppler on lateral and septal annulus, pulmonary vein velocities, E wave to average annular velocity ratio (E/e'), E/A ratio, right ventricular systolic pressure. Mitral inflow analysis was performed by placing the sample volume at the mitral leaflet tips in the apical four chamber view and obtaining continuous and pulsed wave Doppler.2)
Statistical analysis
Continuous variables were expressed as mean and standard deviation (SD); categorical variables were expressed as number and percentage. Difference between groups was assessed with the 2-sample t-test or Wilcoxon rank sum test for continuous data. For categorical data, the χ2 test was used. Linear regression was used to determine whether the E/A correlated with the E/e'. Receiver operating curves and optimal sensitivity and specificity cutoff points were chosen using logistic regression models. Corresponding 95% confidence intervals (CI) were derived using standard binomial distribution methods. A p value less than 0.05 was considered statistically significant. All analyses were performed using JMP version 8.0.2 software (SAS Institute Inc., Cary, NC, USA).
Results
Baseline characteristics of the case patients are shown in Table 1. The mean age of the controls was 70 ± 8 years versus mean age in cases was 69 ± 8 years (p = 0.94). Of note, many patients with severe MR were asymptomatic (40%) at surgery, however met the criteria suggested by the American College of Cardiology to undergo surgery.8) All patients had elective surgery and the median duration between the echocardiogram and cardiac surgery was 54 days. Only one patient had an echocardiogram done the day of his elective cardiac surgery and it was done to reconfirm the severity of MR that noted on his echocardiogram 11 months prior. Mean (SD) MR volume was 80 (17) mL and the effective regurgitant orifice was 0.51 (0.14) cm2 in case patients. Table 2 shows no significant difference in age and EF among case patients and control subjects. Left ventricular end-diastolic dimension and left ventricular end-systolic dimension were greater in cases than controls, as expected. Our study population consisted of 71% males and 29% females and the male population had a higher left ventricular end-diastolic dimension (LVEDD) (56 ± 7 mm) (mean ± SD) when compared to females where the mean LVEDD (50 ± 7 mm) (mean ± SD) (p = 0.04). In addition, average E wave velocity was significantly higher in the case patients than control subjects (Table 2), as were the left atrial volume index and right ventricular systolic pressure.
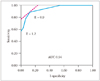
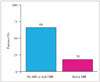
Among patients with severe MR, mitral E wave velocity was less than 1.2 m/sec in 43% (95% CI, 28-59%) (Fig. 1). Echocardiographic images and Doppler findings of a patient who had severe MR due to flail leaflet quantified by PISA method who underwent mitral valve surgery are shown in Fig. 2. Despite severe MR, mitral inflow Doppler showed an E wave velocity of < 1.2 m/sec (Fig. 2D). Receiver operator curve showed that, although E wave velocity of more than 1.2 m/sec is highly specific (100%; 95% CI, 90-100%), it has low sensitivity (57%; 95% CI, 41-72%) to diagnose severe MR (Fig. 3). The optimal cutoff value of the E wave velocity was 0.9 m/sec, which has a sensitivity of 89% (95% CI, 74-95%) and a specificity of 86% (95% CI, 71-94%). An A wave dominant mitral inflow pattern was observed in 18% (95% CI 9-34%) of the case patients with severe MR; although the percentage of control subjects with an A wave dominant mitral inflow pattern was significantly higher (66%; 95% CI, 49-79%) (p < 0.001) (Fig. 4).
We also compared the mitral annular areas (using diameters measured at the onset of atrial contraction from the apical 2 and 4 chambers and assuming that the annulus is an ellipse) in patients with severe MR who had E wave velocities of 1.2 m/sec or greater to those who had E wave velocities of less than 1.2 m/sec. We found no significant difference between the mitral annular areas in these groups [40.0 (7.0) cm2 vs. 40.0 (12.0) cm2; p = 0.98].
When examining mitral regurgitant volume in those patients
with severe MR and an E wave velocity greater than 1.2 m/sec and those who had severe MR and an E wave velocity less than 1.2 m/sec there was no significant difference in the regurgitant volume between the 2 groups: 81 (16) mL vs. 78 (19) mL, respectively (p = 0.61).
Discussion
Our study, consisting of patients with quantified severe chronic, organic, quantified mitral valve regurgitation due to either flail mitral valve leaflets or mitral valve prolapse requiring surgery, shows that although E wave velocity of 1.2 m/sec is highly specific for severe organic MR, it is not sensitive enough (57%) to exclude severe MR and thus is less likely to be useful as a screening tool. An E wave velocity of 0.9 m/sec may be more useful because of optimal sensitivity (89%) and specificity (86%). In addition, an A wave-dominant pattern alone cannot exclude patients with severe organic MR because 18% of patients with severe MR in our study were found to have an A wave-dominant pattern.
MR is a progressive disease and the timing of surgery is crucial since delaying mitral valve surgery can lead to left ventricular dysfunction and decreased long-term survival.9-11) In fact, the American College of Cardiology states that surgery should be considered even in asymptomatic patients who meet certain criteria.8) Similarly the European Society of Cardiology guidelines suggest that the management of asymptomatic patients with mitral valve regurgitation is controversial, however these patients require careful serial follow-up and surgery should be considered early once certain parameters are met.12) Thus, a reliable, yet efficient, method is crucial for quantifying the severity of MR.
Several qualitative measures have been proposed, including continuous wave Doppler jet density and pulmonary vein flow patterns.3) Quantitative methods include calculation of regurgitant volume and effective regurgitant orifice area.3) Although these methods are well validated in several studies, they are time consuming and may not be the ideal screening method for excluding patients with severe MR.
Early mitral inflow velocity reflects the instantaneous pressure difference between the left atrium and the left ventricle.13) In severe MR, the pressure gradient between the left atrium and left ventricle increases and leads to a higher peak E wave velocity. However, several other factors also affect E wave velocity, such as preload, blood pressure, rate of relaxation of the left ventricle, compliance of both the left atrium and the left ventricle, and the left ventricular end-systolic volume.14-16) The clinician cannot truly rely on E wave velocity in excluding those with severe MR.
In a similar manner, the left atrium of young, healthy patients can contribute as much as 30% to left ventricular filling during diastole.16) On pulsed wave Doppler, the A wave (associated with atrial contraction) has been shown to increase with aging, including a decrease in E/A ratio due to impaired left ventricular relaxation.17) However, it also has been proposed that A wave dominance virtually excludes severe MR.2)
A study by Thomas et al.2) found that a peak mitral inflow velocity of more than 1.2 m/sec identified patients who had severe MR with a sensitivity of 85% and a specificity of 86%. This study also found that no patient with severe MR had an A wave-dominant mitral inflow pattern. However, their study did not specifically include many patients with severe MR due to flail mitral valve leaflets or mitral valve prolapse requiring surgery (n = 8). In contrast, our study included only patients with quantified severe MR due to flail mitral valve leaflet or mitral valve prolapse (as seen during surgery) (n = 35). Our analysis showed that E wave velocity of 1.2 m/sec has good specificity, yet poor sensitivity, in predicting severe MR. In fact, our study showed that an E wave velocity of 0.9 m/sec has better sensitivity and specificity overall in predicting severe MR.
To understand why severe MR results in an E wave velocity less than 1.2 m/sec and to determine if perhaps an enlarged annulus could contribute to these findings, we compared the mitral annular areas (using diameters measured at the onset of atrial contraction from the apical 2 and 4 chambers and assuming that the annulus is an ellipse) in patients with severe MR who had E wave velocities of 1.2 m/sec or greater to those who had E wave velocities of less than 1.2 m/sec. We found no significant difference between the mitral annular areas in these groups.
We also examined the mitral regurgitant volume in those patients with severe MR and an E wave velocity greater than 1.2 m/sec and those who had severe MR and an E wave velocity less than 1.2 m/sec. It may be that both E wave velocity and mitral inflow pattern (E/A) are affected by other factors, such as diastolic function and age so that in some patients, E wave velocity of 1.2 m/sec and a mitral A wave dominant pattern cannot be used as the sole factors to exclude severe MR. From a clinical standpoint, physicians should not be using an absolute value of 1.2 m/sec for the mitral E wave velocity and the A wave dominant mitral inflow pattern alone to exclude severe MR. It is prudent to not only look at the valve anatomy but to also perform comprehensive quantitation in patients with moderate or greater MR.
Our study sample was relatively small; it consisted of 35 patients with severe MR because we wanted to include only patients with severe MR due to flail mitral valve leaflets or mitral valve prolapse requiring surgery. Also we wanted to include only those patients with EF greater than 60%, those who were not paced and in normal sinus rhythm, and exclude patients who had MR from causes other than pure organic reasons (flail or prolapse), and those who did not have any other valvular diseases. This reduced our sample size down from the initial 300 patients that were screened. Thus, larger scale studies are needed to confirm our findings. However this study highlights the importance of not relying on a few parameters to evaluate severe MR and emphasizes the fact that patients should be comprehensively evaluated for severity of MR to determine timing of surgery.
In conclusion, although E wave velocity of 1.2 m/sec is highly specific for severe organic MR, it is not sensitive enough. Thus, E wave velocity of 0.9 m/sec may be more useful because of optimal sensitivity and specificity. An A wave-dominant pattern alone cannot exclude patients with severe organic MR. Our findings underscore the importance of a comprehensive echocardiographic evaluation of MR rather than relying on one or two simple Doppler measures which sometimes may be misleading.




 XML Download
XML Download