

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Ankylosing spondylitis (AS) is a chronic systemic inflammatory disorder that usually begins at the age of approximately 26 years, presents more often in men than women, and mainly affects the axial skeleton.1) Among the well known extra-articular involvements in AS, cardiac involvements which include aortitis, aortic insufficiency, conduction disturbance, and myocardial involvement are found in some patients.2-5) The most prevalent manifestations are aortic regurgitation and conduction defects, and these are generally limited to the aortic root area.3-7) Although recent therapy for AS has advanced significantly, the prevalence and clinical characteristics of subclinical cardiac involvement in early AS remain unclear.
Methods
Study population
Consecutive AS patients who had been managed at our institution between January 2007 and December 2008 were enrolled in this study. All patients were men and fulfilled the modified New York diagnostic criteria for AS10) and did not have any history or clinical symptoms of cardiac disease. A total of 70 AS patients on treatment were divided into group I (< 10 years) and group II (≥ 10 years) depending on their disease duration after the first diagnosis. Twenty-five healthy volunteers were selected as control subjects and were age-matched to group I. No female AS patient agreed to the study, and were consequently not enrolled. Patients were excluded if they were older than fifty because of possible degenerative valve disease11)12) and other potential combined rheumatologic diseases. This study was approved by the ethics committee of our institutional review board and all subjects gave informed consent.
Rheumatologic evaluation
The clinical evaluation included structured interview, routine blood test, and conventional X-ray. Interview included age at onset of first symptoms and diagnosis. In addition, medical information concerning low back pain and spinal stiffness (duration, severity), history of anterior uveitis, hip joint pain, and number of inflamed peripheral joints was obtained. We also assessed medical records for other missed history or events, as well as history of anti-tumor necrosis factor therapy (etanercept). Routine blood tests were performed, and patients were screened for human leukocyte antigen B27, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and immunoglobulin A (Ig A) for disease activity or inflammatory markers.1)13) Spinal joint and hip (sacroiliac joint) involvement was assessed by conventional radiology, whereas disease activity and functional ability were assessed by the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI).14)15)
Echocardiography and electrocardiography
All patients underwent TEE uneventfully after TTE using the iE33 machine (Philips Medical Systems, Eindhoven, Netherlands) with a high resolution TEE probe (S7-2 Omni) and TTE probe (S5-1), conducted by an experienced cardiologist blinded to the clinical data. Blood pressure (BP) was measured by a sphygmomanometer while the subject was in a supine position, before and after performing TEE.
To evaluate cardiac structure (left atrial size, left ventricular mass), systolic function [left ventricular ejection fraction (LVEF)] and diastolic function [deceleration time of mitral inflow, the ratio of the peak mitral velocity of the early rapid filling wave (E) and mitral annulus early diastolic velocity (E')], were studied using TTE including pulsed wave tissue Doppler imaging to record mitral annular velocity for myocardial velocity as previously recommended.16-19) LVEF was calculated by the modified Simpson's method.16)
Aortic root diameter at annulus, sinus of Valsalva (SOV), and sino-tubular junction, the end diastolic ascending aortic diameter, aortic valve thickness (at the mid portion of non-coronary cusp) and mitral valve thickness (at the basal portion of anterior leaflet) were measured on the long axis view of 2-dimensional based TEE images (Fig. 1).16) Mitral or aortic valve regurgitation was assessed and graded by widely accepted criteria using color flow Doppler imaging.17) After measurement of both diastolic and systolic diameters of descending thoracic aorta by M-mode, aortic stiffness and aortic elasticity indices were calculated as follows:20)21)
• Aortic strain (%) = (systolic diameter of aorta - diastolic diameter of aorta) × 100/diastolic diameter
• Aortic distensibility (cm2dyn-1 × 10-3) = 2 × aortic strain / (systolic BP - diastolic BP)
• Aortic stiffness beta index = ln (systolic BP/diastolic BP) / [(systolic diameter of aorta - diastolic diameter of aorta) / diastolic diameter]
All measurements were averaged over three cardiac cycles, and all subjects had 12-lead electrocardiography (ECG). One board certified cardiologist interpreted the ECG.
Statistical analysis
All descriptive measurements were expressed as mean ± SD. Differences between groups were compared using independent samples t-test, or Chi-square test as appropriate. A subset analysis of patients was done by one-way ANOVA using the Tukey method as a post hoc test. Correlations between variables were determined by the Pearson correlation coefficient (r). To find the independent predictors of aortic valve thickening among clinical variables, logistic regression analysis was done. Receiver operating characteristics (ROC) curve analysis was performed to assess the aortic valve thickness predicting AS. Statistical significance was considered with a p value of < 0.05. All tests were two-tailed. Statistical analysis was performed using the SPSS vs.13.0 software package (SPSS, Chicago, IL, USA).
Results
Clinical characteristics
A total of 70 AS patients on treatment without clinical cardiac symptoms were divided into group I (< 10 years, n = 50, mean age 26.7 ± 4.8 years) and group II (≥ 10 years, n = 20, mean age 33.9 ± 5.8 years) depending on their disease duration after first diagnosis (Table 1).
Except for the older age in AS group II than the control and AS group I, there were no significant differences in height, weight, body mass index, systolic and diastolic BP, pulse pressure, heart rate, current smoker status and hypertension among the subjects. Five AS patients (5/70, 7%) had a history of hypertension or were under treatment for it. No patient with AS had conduction disturbance, ischemic changes, and other significant arrhythmias on 12-lead ECG. Also, no significant differences in PR interval, QTc interval, and QRS duration were found in both the control and AS group.
Symptom duration (from the onset of symptoms to first diagnosis) and disease duration were longer in AS group II (14.0 ± 4.8 years, 2 to 25 years; 13.4 ± 3.0 years, 10 to 18 years, respectively) than AS group I (4.2 ± 2.8 years, 0 to 12 years; 3.2 ± 2.2 years, 0 to 8 years, respectively) (p < 0.001, respectively). Sixty-two (89%) (45/50, 90% in AS group I; 17/20, 85% in AS group II) of 70 AS patients were positive for human leukocyte antigen B27. AS group II had more elevated ESR and CRP, and higher prevalence of hip involvement and history of etanercept use. There was no significant difference in BASDAI and history of uveitis and peripheral joint involvement between the AS group I and AS group II.
Echocardiographic characteristics
Table 2 shows the echocardiographic data. Cardiac structure (left atrial size, left ventricular mass), LVEF, global function (Tei index), and diastolic function (deceleration time of mitral inflow, E/E') did not show significant differences between the groups. Tissue Doppler imaging to record mitral annular velocity for myocardial velocity revealed more decreased early diastolic (E') and systolic (S') velocities in AS group II compared to AS group I, and were also more decreased in AS group II than the control group for E' velocity. There was no significant differences in E' (11.8 ± 1.3 vs 11.0 ± 1.8, p = 0.061) and S' (8.6 ± 1.2 vs. 8.1 ± 1.2, p = 0.076) between the controls and the AS patients.
Aortic root diameter at the annulus (20.4 ± 1.6 vs. 20.5 ± 1.4 mm, p = 0.738), SOV (30.7 ± 2.7 vs. 31.0 ± 3.3 mm, p = 0.708), and sino-tubular junction (24.2 ± 2.3 vs. 24.4 ± 2.1 mm, p = 0.605) were not different significantly between the controls and AS group. AS group II showed an increased aortic root diameter at the SOV and at the sino-tubular junction compared to AS group I. Ascending aortic diameter was more increased in AS group II than in both AS group I and the controls.
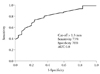
The thickness of both the aortic and mitral valve was more increased in both AS groups than in the controls. The prevalence of aortic and mitral regurgitation was not different between the controls and the patient groups (0% vs. 1.4% for aortic; 4% vs. 5.7% for mitral). ROC analysis showed that aortic valve thickness over 1.3 mm could predict AS with a sensitivity of 73%, specificity of 76%, and area under the curve of 0.8 (95% confidence interval, 0.707-0.887; p < 0.001) (Fig. 2). Aortic valve thickening was defined with this cut-off value > 1.3 mm. The prevalence of aortic valve thickening was higher in the AS groups (54/70, 77%) than in the controls (9/25, 36%) (p < 0.001).
Aortic strain, aortic distensibility, and aortic stiffness beta index were more decreased in AS group II compared to other groups. There was no significant differences in aortic strain (13.1 ± 3.0% vs. 12.7 ± 4.1%, p = 0.602), aortic distensibility (0.6 ± 0.2 vs. 0.5 ± 0.2 cm2dyn-1 × 10-3, p = 0.589) and aortic stiffness beta index (2.5 ± 0.3 vs. 2.6 ± 0.3, p = 0.357) between the controls and both AS groups.
Aortic valve thickening and related clinical variables
On univariate analysis using Pearson correlation, no clinical variable was found to be related to mitral valve thickness. Aortic valve thickness was significantly related to systolic BP (r = 0.204, p = 0.047), disease duration (r = 0.329, p = 0.005), BASDAI (r = 0.342, p = 0.044), ESR (r = 0.483, p < 0.001), CRP (r = 0.495, p < 0.001), and Ig A (r = 0.292, p = 0.014). However, on both linear and binary logistic regression analysis, an independent predictor for aortic valve thickening was not found among the clinical variables that had shown significance on univariate analysis.
Discussion
This study showed that both aortic and mitral valve thickening without regurgitation were noted in young male AS patients even without cardiac symptoms early in the course of their disease. To our knowledge, this is the largest study to evaluate the subclinical cardiac valve disease in early AS using TEE.
Comparison with previous echocardiographic studies
The cardiac abnormalities in AS may have been overestimated in the past, compared with the results of our study. When examined by high resolution TEE, only aortic and mitral valve thickening were noted as early changes in young AS patients, and the prevalence of aortic and mitral regurgitation was very low with no difference between the controls and patients (0% vs. 1.4% for aortic; 4% vs. 5.7% for mitral). Roldan et al.5) examined the aortic root and valve in 44 AS patients with a mean disease duration of 20 (± 11) years and in 40 patients by TEE. They found aortic root and valve disease in 82% of AS patients compared to the controls (27%). These discrepancy between previous study and our data maybe in part explained by remarkable development in anti-inflammatory therapy including anti-tumor necrosis factor therapy. Brunner et al.22) studied 100 male subjects with AS and a disease duration of more than 15 years using ECG and TTE. In patients with long-standing AS, there was no increased rate for valve regurgitation (mitral and aortic valve) and for arrhythmia. We also found that the incidence of valve regurgitation was not different from normal controls, and conduction abnormalities or arrhythmia was not discovered in AS patients if the disease duration was short (< 10 years).
Changes of aortic root and ascending aorta
Aortic root diameter at the SOV and at the sino-tubular junction and ascending aortic diameter increased to a greater extent in the older AS patients than in the younger AS patients. Although young AS patients did not show significant differences in aortic elasticity index (aortic strain, aortic distensibility) and aortic stiffness (beta index) as compared to the controls, older AS patients (defined as group II in this study) had more decreased aortic elasticity and increased stiffness than the controls. A previous study to determine the aortic elasticity in 35 AS patients (younger than 40 years) using TTE at the ascending aorta found that aortic elasticity decreased in AS patients and this decrease was not related to the disease duration.23) Compared to this study, we used TEE with the advantage of providing closer views of the aorta and aortic valve, and more detailed definition of thoracic aortic diameter than the TTE.8)9)24) The lack of sensitivity of TTE to detect cardiac abnormalities was also stressed in another study using TEE in 29 male AS patients and 13 controls.8)
Factors related to increased aortic diameter and decreased aortic elasticity in older AS patients in our study may be complex because it has been known that there are many factors affecting aortic stiffness and aortic diameters including age, hypertension, obesity, and smoking.12)25) It was also reported that AS was associated with subclinical atherosclerosis and arterial stiffness.26) However, our results did not show the association between CRP or ESR and valvular thickening. Recent studies have focused on vascular pathologies and showed impaired endothelial function, suggesting that atherosclerotic alterations could also be involved in increased cardiovascular mortality.27)28)
Ventricular function in ankylosing spondylitis
Myocardial failure due to left ventricular dysfunction may occur in AS patients.3)28-31) In our study it was noteworthy that we used tissue Doppler imaging, which can detect myocardial function with greater sensitivity,18)19) revealing no change in myocardial function in early AS patients. However, older AS patients showed depressed left ventricular function as identified by decreased myocardial velocities (E' and S') compared to the controls. Whether these differences were due to AS itself or to a higher prevalence of cardiovascular risk factors in older patients remains to be determined, and was beyond the scope of the present study.
There are some limitations in this study. First, our study was conducted in a single center of Korea. Selection bias inherent to this may be unavoidable. In addition, because the subjects were not selected from a nation-wide registry, only small numbers were recruited, which could imply that these results may not be expandable to other populations. Second, no female AS patients agreed to the study, which meant we had to conduct the study only in male patients. Third, the design of our study was observational and not prospective. The evolution of early changes in aortic valve and root should be followed up in a larger long-term prospective study. Fourth, we did not get any pathologic specimen which may provide information about the pathogenesis of valvular thickening in AS patients.
Conclusion
Both aortic and mitral valve thickening without regurgitation were noted in male AS patients early in the course of their disease even without clinical cardiac manifestations. This subclinical change of the aorto-mitral valve in early AS should be considered and followed up to determine its prognostic implication and evolution.



 XML Download
XML Download