

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Atrial fibrillation (AF) is the most frequently detected arrhythmia in the clinical setting, and is associated with increased cardiovascular risk.1)2) AF is a progressive condition that begins with hemodynamic and/or structural changes in the left atrium (LA) and evolves through the paroxysmal and persistent stage.3) Better understanding of LA structure and function could lead to improvements in our ability to predict the risk of developing AF and the response to treatment in patients with this arrhythmia. LA enlargement has been widely related to AF, both in patients with chronic AF and in those with paroxysmal AF.4-6) Over the past decade, there has been increasing interest in the noninvasive evaluation of LA size and mechanical function. LA function can be estimated by two-dimensional echocardiography, Doppler analysis of transmitral flow, and tissue Doppler assessment of LA myocardial velocities. Speckle tracking echocardiography allows the quantification of LA function, and recently, noninvasive estimate of LA strain by speckle tracking has been proposed.7) Several studies have shown that LA stiffness increases with atrial remodeling and reflects a deteriorated reservoir function.7)8) However, to date, little is known with regard to the change of LA mechanical function, including LA stiffness, in patients with AF. In this study, we tried to determine the contribution of LA mechanical function, including LA stiffness, to AF by comparing the paroxysmal AF patients with normal control subjects, and to evaluate whether LA mechanical function and stiffness are related with structural changes of LA.
Methods
Study population
We conducted a multicenter, prospective, case-control study. The study population included 64 patients [mean age, 57 ± 13 years; male, 59%; mean left ventricular (LV) mass index, 88 ± 21 g/m2] with paroxysmal AF who underwent echocardiography for the evaluation of cardiac structure and function, between June 2006 and October 2007. Inclusion criteria were as follows; 1) age older than 18 years, 2) recent onset and documented AF on an electrocardiogram or Holter recording in the previous 2 months, and 3) sinus rhythm at the time of the echocardiographic examination. Patients were excluded from the study if any of the following were present; 1) prior history of AF, 2) LV ejection fraction < 50%, 3) history of ischemic heart disease, 4) dyspnea of New York Heart Association functional class ≥ II, 5) valvular stenosis or regurgitation ≥ moderate, and 6) hyperthyroidism, acute illness, post-operative status. Thirty six healthy subjects with similar age, gender, and LV mass index distribution (mean age, 53 ± 14 years; male, 61%; mean LV mass index, 86 ± 18 g/m2) were randomly selected from the subjects who volunteered for general routine health evaluation and underwent echocardiography. None of the controls had any cardiovascular or systemic disease and had sinus rhythm. The institutional review board approved the study protocol.
Transthoracic echocardiography
A Vivid 7 ultrasound system (GE Vingmed Ultrasound, Horten, Norway) was used for the transthoracic echocardiographic examination. All images and measurements were acquired from the standard views, according to the guidelines of the American Society of Echocardiography9-11) and were digitally stored for offline analysis. In the parasternal long-axis views, LA maximum anterior-posterior (A-P) diameter was measured. In the apical 4-chamber view, LV end-diastolic and end-systolic volumes were measured and LV ejection fraction was calculated by the Simpson method. In the same view, LA superior-inferior (S-I) diameter was measured from the mitral annular plane to the posterior wall of the LA, and velocity time intergral of A wave (VTIA) was measured. Pulsed-wave Doppler at the tip of mitral valve leaflets allowed us to measure the early (E) and late (A) diastolic filling velocities, E/A ratio, and E deceleration time. The LV tissue velocity (e', a', s') were measured by tissue Doppler imaging of the medial mitral annulus and E/e' was calculated. From the apical 4- and 2-chamber view, the following LA volumes were measured using a biplane area-length method, and were indexed to body surface area: maximum volume (before mitral valve opening), pre-A volume (before atrial contraction), and minimum volume (after atrial contraction). LA reservoir function was estimated by the LA expansion index (%), computed as [(LA maximum volume - minimum volume) / minimum volume] × 100%. LA contractile function was estimated by the LA active emptying fraction (%), computed as [(LA pre-A volume - minimum volume) / pre-A volume] × 100%. LA ejection force (kdynes.cm/m2) was calculated according to the modified Manning method as (0.5 × ρ × LA active emptying volume index × A2) / VTIA, where ρ is blood density of 1.06 g/cm3, A is peak late diastolic transmitral flow velocity (cm/sec), and VTIA is late diastolic transmitral flow velocity time integral (cm).12) LA kinetic energy (kdynes/m2) was defined as 0.5 × ρ × LA active emptying volume index × A2.
The global systolic LA myocardial strain was measured by 2-dimensional speckle tracking echocardiography.8) Gray scale image of apical 4-chamber views was obtained with the frame rates of 50-80 Hz. Recordings were processed with acoustictracking software (EchoPAC, GE Healthcare, Horten, Norway), allowing off-line semi-automated speckle-based strain analyses. Briefly, the lines were manually traced, along the LA endocardium at the time of end-systolic phase. An additional epicardial line was automatically generated by software, which created a region of interest (ROI). After manually adjusting the ROI shape, the global peak LA strain during the whole cardiac cycle was calculated.13)14) In this study, to derive a noninvasive dimensionless parameter, the ratio of E/e' to LA peak strain was used to estimate the LA stiffness (Stiffnessstrain).7)8) We also estimated LA stiffness as the ratio of E/e' to LA filling volume (Stiffnessvol).
Statistical analyses
Continuous variables are expressed as the means and standard deviations; categorical variables are expressed as proportions. The Student t-test was used to test for the differences in normally distributed continuous variables, and the Wilcoxon rank sum test was used for comparisons involving the variables that were not normally distributed. Categorical variables were compared with the χ2 test or Fisher exact test as appropriate. A two-sided p-value of less than 0.05 was considered to represent a statistically significant difference. The correlation between LA stiffness and LA volume indices and mechanical function indices were evaluated using Pearson's correlation coefficient (PCC) and Spearman's rank correlation coefficient (SCC).
Results
The baseline clinical and echocardiographic characteristics of 64 patients with paroxysmal AF and 36 normal control subjects are summarized in Table 1. There was no significant difference between the paroxysmal AF patients and normal control subjects, with respect to age, gender, heart rate, and body surface area (Table 1). Although LA A-P diameter was not significantly different between the two groups (3.7 ± 0.6 vs. 3.5 ± 0.5, p = 0.207), S-I diameter was increased in patients with paroxysmal AF, compared to the normal control subjects (5.2 ± 0.8 vs. 4.8 ± 0.5, p = 0.002). LA volumes were also significantly larger in the paroxysmal AF patients than in the normal control subjects (minimal volume index, 16.6 ± 8.8 vs. 10.6 ± 4.6, p < 0.001; pre-A volume index, 22.3 ± 9.9 vs. 15.9 ± 6.5, p = 0.001; maximal volume index, 33.2 ± 11.4 vs. 26.7 ± 8.8, p = 0.004). Whereas, there was no significant differences in LV volume and mass indices, transmitral flow velocities and annular tissue velocities between the two groups (Table 1).
Table 2 describes the LA mechanical function in patients with paroxysmal AF and in the normal control subjects. The reservoir function, as estimated by LA expansion index, was significantly decreased in patients with paroxysmal AF, compared to that of the normal control subjects (118.1 ± 50.5 vs. 164.5 ± 54.4, p < 0.001). Whereas, decreased contractile function in patients with paroxysmal AF, as estimated by LA active emptying fraction, did not reach statistical significance (26.5 ± 12.8 vs. 31.7 ± 13.7, p = 0.056). There was no significant difference in LA energy, including kinetic energy (7.7 ± 7.6 vs. 6.6 ± 5.2, p = 0.449) and ejection force (1.1 ± 0.8 vs. 1.0 ± 0.7, p = 0.540) between the two groups. Paroxysmal AF patients showed lower global LA strain (27.3 ± 7.2 vs. 32.6 ± 7.0, p = 0.001) and higher LA stiffnessstrain (0.41 ± 0.24 vs. 0.29 ± 0.10, p = 0.001), compared to normal control subjects. However, when we estimate LA stiffness, using LA filling volume, LA stiffnessvol was not significantly different between two groups (0.68 ± 0.38 vs. 0.63 ± 0.26, p = 0.543).
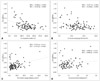
Fig. 1 illustrated correlation between LA stiffnessstrain and LA volume indices. In the overall study population, the LA stiffnessstrain was strongly correlated with LA minimal (PCC = 0.702, p < 0.001; SCC = 0.467, p < 0.001), pre-A (PCC = 0.604, p < 0.001; SCC = 0.410, p < 0.001), and maximal volume indices (PCC = 0.523, p < 0.001; SCC = 0.388, p < 0.001) (Fig. 1). Fig. 2 illustrated correlation between LA stiffnessstrain and LA mechanical function indices. LA expansion index showed a negative correlation with LA stiffnessstrain (PCC = -0.484, p < 0.001; SCC = -0.429, p < 0.001) (Fig. 2A). LA active emptying fraction also showed a negative correlation with LA stiffnessstrain (PCC = -0.357, p < 0.001; SCC = -0.298, p = 0.003) (Fig. 2B). LA kinetic energy showed a weak correlation with LA stiffnessstrain (PCC = 0.255, p = 0.011; SCC = 0.201, p = 0.048), but LA ejection force did not show a significant correlation with LA stiffnessstrain (PCC = 0.085, p = 0.451; SCC = 0.086, p = 0.445) (Fig. 2C and D).
Discussion
The main findings of our study are that patients with paroxysmal AF showed a decreased reservoir function, rather than contractile function, and increased stiffness compared to the control subjects. LA stiffness was strongly correlated with LA volume indices and moderately correlated with atrial reservoir and contractile function. Paroxysmal AF may constitute a good model to study. If there is any anatomical or functional substrate in these patients with apparently normal hearts, those changes may promote the development of persistent or permanent AF. The importance of atrial enlargement in the development of AF is well-known.4-6) Sitges et al.6) found that LA enlargement was observed already in patients with paroxysmal AF. In this study, maximal LA dimensions, area and volume are significantly larger in patients with AF, when compared with the healthy volunteers without AF. Our results are in accordance with their findings on LA enlargement. Not only LA maximal volume, but also pre-A and minimal volumes were increased in the paroxysmal AF patients.
To date, little is known in regard to the role of LA function in the development of AF. In the current study, we found that LA reservoir function, as estimated by LA expansion index, was significantly decreased in patients with paroxysmal AF, compared to that of the normal control subjects. However, the difference in LA contractile function, as estimated by LA active emptying fraction, between the two groups did not reach a level of statistical significance. Although the role of LA mechanical function in the progression of AF was not examined in this investigation, a previous prospective study has shown that reduced LA reservoir function, as estimated by LA total emptying fraction, was a robust predictor of first AF or atrial flutter, which was superior and incremental to the maximum LA volume.15)
Recently, strain analyses with two-dimensional speckle tracking echocardiography have been applied to the LA.13)14) LA myocardial strain has been confirmed as a reliable index that represents the magnitude of atrial deformation.16) LA strain during LV systole indicates the LA reservoir function, and lower measurement value of it suggests a deteriorated LA function and progression of LA remodeling.8) In a previous study by Henein et al.,17) global LA strain and strain rate were significantly reduced in patients with paroxysmal AF, compared with the normal control subjects. We also found the decreased global LA strain in the paroxysmal AF patients. In a previous study by Kurt et al.,7) the use of LA strain, with LA pressure to estimate LA stiffness, has been reported. The authors also suggested the noninvasive estimation of LA stiffness by using the E/e' ratio in conjunction with LA strain. In the study, noninvasively measured LA stiffness, as well as invasively measured LA stiffness, were increased in patients with diastolic heart failure. In the current study, we found that the noninvasive estimate of LA stiffness was significantly increased in patients with paroxysmal AF, compared to those without AF. In addition, LA stiffness was correlated with LA volume indices and reservoir function.
This study has several limitations. First, despite the compared groups of the paroxysmal AF patients and healthy controls had similar distribution of age, gender, and LV mass index, they were not strictly matched. Therefore, difference in LA size and function could be partially influenced by age, which was slightly older (mean difference, 4 years), although not statistically significant, among patients with paroxysmal AF. However, the absence of any significant difference in LV diastolic function parameters suggests that this slight difference in age may not play a role in the large size and decreased mechanical function of LA in the AF group. Second, we compared paroxysmal AF patients only with the normal control subjects. Absence of the persistent/permanent AF group did not allow the evaluation of LA mechanical function, according to the progression of AF to chronic stage. In addition, this is the cross-sectional study; thus, we were not able to determine whether LA mechanical function including LA stiffness can predict the progression to chronic AF. Further study is required to evaluate the predictive value of LA stiffness or other mechanical function for the progression of AF.
In conclusion, patients with paroxysmal AF have decreased LA reservoir function and increased stiffness in comparison with the control subjects. LA stiffness was significantly related with LA volume indices and reservoir function. Noninvasively measured LA stiffness is expected to be used for the assessment of LA function in patients, but the role of LA stiffness in the progression of AF was remained to be proven.



 XML Download
XML Download