

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Atrial fibrillation (AF) is the most frequently encountered arrhythmia in clinical practice, with an overall prevalence of 0.4% in the general population.1) The prevalence of AF increases with age, occurring in 3.8% of people age 60 years and older and in up to 9% of people over 80-year-of-age.2)3) As the proportion of the elderly in many societies continues to increase, the number of patients with AF will likely increase. AF is associated with the significant clinical problems of systemic thromboembolism and hemodynamic deterioration. Quality of life and exercise capacity are also impaired in patients with AF. Data from the Framingham Heart Study suggest that the presence of AF is associated with a near doubling of both overall and cardiovascular mortality.4) Advances in imaging technology and in the understanding of the pathophysiology of AF are leading to more definitive and potentially curative therapeutic approaches. Among the various diagnostic tools, echocardiography has an important role in the evaluation of cardiac structure and function and risk stratification in AF. Two-dimensional (2D) and Doppler study using transthoracic echocardiography (TTE) should be performed for the initial workup of all patients with AF, in order to acquire information about left atrium (LA) and left ventricle (LV) size and function, and the presence of valvular, myocardial, pericardial and congenital heart disease which may predispose to AF. Echocardiography has also become an essential part of the guidelines for management of patients with AF,5) especially in elucidating the mechanisms of systemic thromboembolism in AF. Recently, the development of intracardiac echocardiography (ICE) has allowed the real-time guidance of percutaneous interventions, including radiofrequency catheter ablation (RFCA) of foci in the pulmonary veins (PV) and left atrial appendage (LAA) closure procedures for patients with AF. In this article, we review the role of echocardiography in the evaluation and management of patients with AF.
Go to : 
Evaluation of LA Size and Function in AF
Anatomical assessment of LA
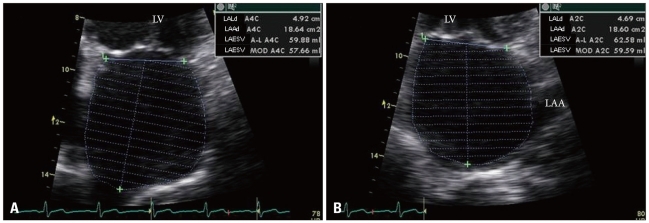
TTE is a reliable method to assess the anatomy of the LA. The measurement of LA anteroposterior diameter from M-mode echocardiography in the parasternal long-axis or short-axis window is commonly utilized in clinical work. This conventional method has a tendency to underestimate true LA size, because the shape of the LA is not spherical and enlargement of the LA is often asymmetrical.6) Hence, 2D derived LA volume assessment using the biplane area-length method or the Simpson's method provides more accurate measures of LA size.7) A horizontal line needs to be drawn across the mitral annular plane, and the LA area does not include the funnel of the mitral valve leaflets (Fig. 1). When tracing the outline of the LA, the LAA and the confluence of the PVs are excluded from the measurement. The reference value for 2D echocardiographic maximum LA volume indexes is 22 ± 6 mL/m2.7)8) A LA volume index of 29 mL/m2 is usually considered the upper limits of the normal value.7) More recently, three-dimensional (3D) echocardiography for assessing LA volume has been available and has demonstrated good correlation with biplane 2D measurements.9) However, studies on 3D echocardiographic measurement of LA volume have been too small, and there is no consensus on the methods or comparisons with established normal values. LA size has been established as a prognostic marker for both adverse cardiovascular events as well as overall outcomes.10-12) According to the data from the Framingham study, a 5-mm increase in LA dimension was associated with a 39% increased risk for subsequent development of AF.4) Psaty et al.13) demonstrated that subjects in sinus rhythm with a LA dimension over 5.0 cm had about four times the risk of developing AF during the following period of surveillance. Increased LA volume, likewise LA dimension, is predictive of subsequent AF11) and it has been confirmed that LA volume is a superior measure over LA dimension for predicting outcomes of AF.14) LA enlargement is associated with a low probability of successful cardioversion for chronic AF or maintenance of sinus rhythm.15)16) An increased LA volume index can predict recurrence of AF after RFCA.17) Although AF promotes further LA enlargement, cardioversion and maintenance of sinus rhythm may reverse this process. Van Gelder et al.18) reported that after restoration and long-term maintenance of sinus rhythm, echocardiographic atrial dimensions may decrease. Reant et al.19) also demonstrated that RFCA for isolated AF reverse morphological remodeling of the LA after restoration of sinus rhythm.
Functional assessment of LA
In addition to providing information about atrial anatomy, echocardiography is also a potent tool for assessment of atrial function. With the loss of atrial booster pump function in AF, the LA-LV pressure gradient during early LV filling is increased by elevation of the LA pressure to maintain stroke volume.20) Thus, a reduction in both LA compliance and volume has been observed with the onset of AF that further decreases cardiac function and increases the risk of thromboembolism. The change of the LA function in different phases can be evaluated non-invasively by echocardiography, utilizing not only usual methods including transmitral flow and changes in LA area and volume, but also novel techniques such as tissue Doppler imaging (TDI) and strain imaging.
Transmitral inflow patterns by pulsed wave Doppler provides information of LA mechanical function. The peak transmitral inflow velocity of the late diastolic filling wave (A) is commonly used as a measure of LA mechanical function,21) but it cannot be measured in AF because of the absence of the atrial waveform. The peak A wave velocity has been used in the serial follow-up of LA function in patients with AF after cardioversion22) and RFCA.23) The time-velocity integral of the A wave and the atrial fraction (i.e., the ratio of the time-velocity integral of the mitral A wave to that of the total diastolic transmitral flow) may be used as a parameter of LA function.24)
TDI allows the quantification of the low-velocity, high-amplitude, long-axis intrinsic myocardial velocities in both systole and diastole, and provides a relatively load-independent measure of both LV systolic and diastolic function.25) The peak velocity at the mitral annulus in late diastole, following atrial contraction (A' or Aa velocity) can be utilized as a rapid and accurate marker of atrial function.26) The A' velocity correlates with other parameters of atrial function such as peak A velocity of mitral inflow, atrial fraction and atrial ejection force.26) Another study also demonstrated that the tissue Doppler A' velocity correlates with LA fractional area and volume change.27)
Doppler strain and strain rate imaging are derivatives of tissue Doppler velocities. TDI quantifies global tissue motion velocity whereas strain and strain rate represent the extent of local tissue deformation and its rate, respectively (Fig. 2). Strain measures the myocardial deformation during a cardiac cycle, and strain rate measures the tissue velocity gradient within the myocardium. Strain and strain rate imaging may overcome the major limitation of TDI, and may be largely independent of translational effects due to tethering by neighboring myocardial segments.
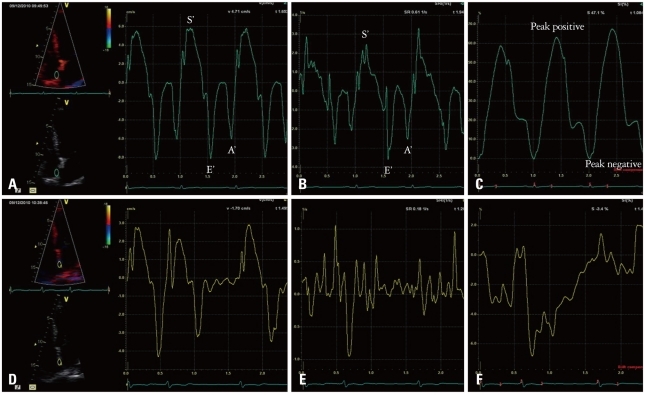 | Fig. 2Representative left atrial (LA) myocardial velocity using tissue Doppler image (TDI), strain rate (SR), and strain curves in a normal subject (A, B, and C, respectively) and a patient with atrial fibrillation (AF) (D, E, and F, respectively). The sample volume is placed at the mid-level of inter-atrial septum. In the patients with AF, no decrease in SR by atrial contraction was observed, but small phasic movements by the AF wave were recorded. Using TDI-derived velocity and SR parameters, it was found that the LA mechanical function was significantly decreased in AF as reflected by reduction in the S' and/or E' wave in the absence of the A' wave during late diastole. S' wave: ventricular systolic wave, E' wave: ventricular early diastolic wave, A' wave: late diastolic wave (atrial contraction).
|
Using TDI and/or strain imaging techniques, it was found the decreased compliance of LA walls, the impairment of the reservoir and conduit function of LA, and the loss of the booster pump function in patients with AF.28)29) With the degree of LA enlargement, LA mechanical dysfunction has emerged as an independent predictors for the maintenance of sinus rhythm after successful cardioversion29) and RFCA.30)
Atrial stunning is characterized by reduced atrial mechanical function after restoration of sinus rhythm from AF, which may last several weeks and which is associated with increased risk of thromboembolism. This phenomenon is well recognized with peak A velocity of transmitral inflow22)24) as well as TDI or strain imaging.31) This suggests that a dissociation of electrical and mechanical recovery occurs after successful restoration of sinus rhythm, with a delay in gradual improvement of atrial mechanical function.
These parameters, mentioned above, can only be easily measured in sinus rhythm and are often not applied to the state of AF. Other LA functional parameters, which are rhythm independent, have been recently suggested as being required.32) More studies and trials to be accepted and validate these parameters are needed to use routinely in clinical practice.
Go to :
Assessment of LV Diastolic Function in AF
The presence and severity of diastolic dysfunction are associated with an increased risk for AF and heart failure in patients with sinus rhythm. Furthermore, the risk for heart failure is markedly increased once AF develops.33) The evaluation of diastolic function in patients with AF has remained a clinical challenge, because the impairment of the LA mechanical function and the variable cycle lengths make the evaluation of diastolic function difficult. Several new methods have been introduced to be useful in measuring diastolic dysfunction of patients with AF. All echocardiographic parameters, which are obtained in the context of AF, should be measured and averaged from 5 to 10 cardiac cycles.
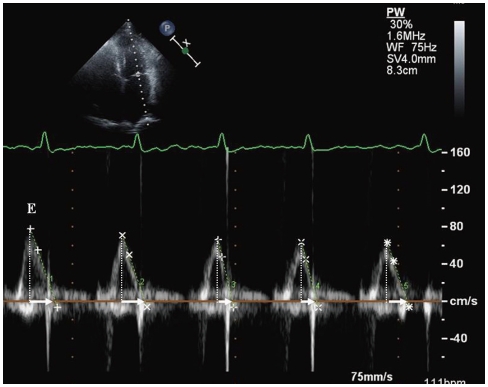
Early transmitral flow deceleration time (DT) provides relatively accurate assessment of LV diastolic function in the setting of AF.34)35) Matsukida et al.36) demonstrated that a cutoff value of mitral DT ≤ 100 ms predicted a mean of pulmonary capillary wedge pressure (PCWP) ≥ 18 mmHg with sensitivity of 80% and specificity 85%. In AF, mitral flow measurements usually include peak LV early diastolic filling velocity (E) and DT over 5 to 10 cardiac cycles. A cycle length equivalent to a heart rate of 60 to 80 beats/min, with the interval ≥ 70 ms between the end of transmitral inflow and the onset of the QRS complex, is preferred (Fig. 3).34)
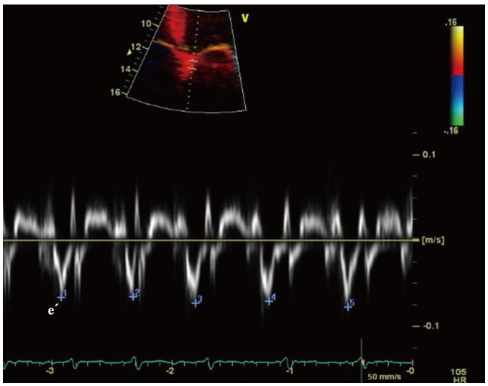
Peak E velocity is dependent on LV relaxation and LA pressure.34) To correct for LV relaxation, peak E velocity can be used as a ratio to the tissue Doppler early diastolic mitral annular motion velocity (e') (Fig. 4). TDI assessment of e' velocity is relatively independent of LA pressure.37) E/e' (septal) > 15 and E/e' (lateral) > 10 have been shown to be highly specific for elevated LV filling pressure.38)39) The E/e' has been validated for LV diastolic filling pressure.40)
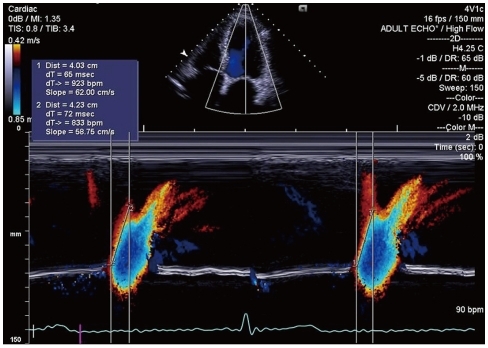
Color M-mode Doppler assessment of mitral inflow propagation velocity (Vp) provides visualization of the temporal and spatial propagation flow along a single scan line from the annulus area to the LA apex throughout the diastolic period. A Vp < 45 cm/s is consistent with the presence of diastolic dysfunction (Fig. 5).41)
The isovolumic relaxation time (IVRT) is the time from the aortic valve closure to the onset of mitral inflow and has been shown to be a strong negative correlation with mean PCWP in AF.34)35) Increased IVRT is a marker of impaired LV relaxation and a shortened IVRT reflects the increased LV chamber stiffness.42)
There may be advantages to the use of regional strain rate imaging for assessment of diastolic function in patients with AF. In AF, there could be regional differences in diastolic filling depending on the LV response to the fibrillating atria. Therefore, regional strain rate imaging is expected to be a promising technique for assessing diastolic dysfunction in AF. However, more studies will be needed before its application to the clinical practice in patients with AF.
Go to :
Pulmonary Venous Flow Assessment in AF
Pulmonary venous blood flow (PVF) exhibits a pulsatile behavior, which is related to LA pressure and function, mitral valve function, and LV compliance. Echocardiography helps to define characteristic flow patterns in AF. The disappearance of atrial reverse flow, a decrease in systolic flow with a greater diastolic than systolic flow, a prolonged onset of systolic flow and the appearance of an early systolic reverse flow are characteristic findings in AF. The disappearance of atrial reverse flow can be explained by the loss of active LA contraction. A decrease in systolic PVF has been also found to correspond closely to LAA dysfunction and spontaneous echo contrast (SEC) formation.43) The change of PVF in AF seems to reflect a alteration in LA function, mainly atrial compliance, and reservoir function.
PVF pattern can be used as a monitoring tool for recovery of LA mechanical function after restoration of sinus rhythm with cardioversion or RFCA. Low systolic PVF obtained during AF (before cardioversion)44) as well as obtained during sinus rhythm (immediately after cardioversion)45) was associated with AF recurrence at 6 and 12 months after electrical cardioversion, respectively. In contrast, an early systolic PVF peak velocity > 57 cm/s predicted good mechanical function recovery with 96% specificity indicating that preserved reservoir function of LA during AF is predictive of satisfactory recovery of mechanical function after PV isolation.46)
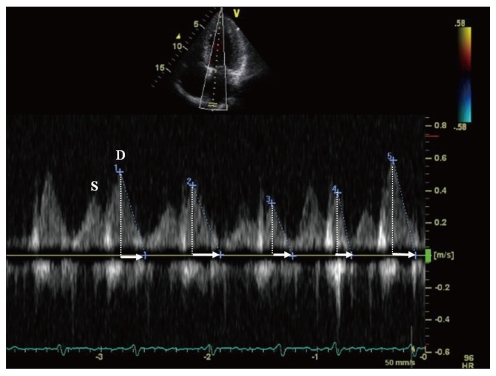
Pulmonary venous diastolic DT is very useful to predict diastolic LV filling pressure, as estimated by PCWP in AF.47) Pulmonary venous DT is calculated as the time between peak diastolic velocity and the upper deceleration slope extrapolated to the zero baseline (Fig. 6). Measurements are usually done in 5 to 10 cardiac cycles, with a cycle length equivalent to heart rate of 60 to 80 beats/min. Pulmonary venous DT correlated better with PCWP than transmitral DT in patients with AF.47) Matsukida et al.36) demonstrated that pulmonary venous DT ≤ 150 ms predicted PCWP ≥ 18 mm Hg with 100% sensitivity and 96% specificity in patients with AF.
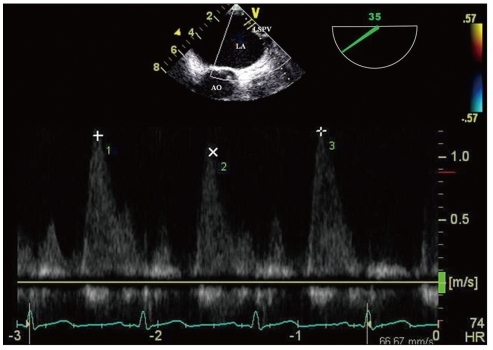
A usage of monitoring PVF is the detection of PV stenosis after RFCA for AF, which occurs in 1% to 3% of current series. The PVF measurements using transesophageal echocardiography (TEE) Doppler have allowed the detection of a significant PV stenosis following RFCA if the diagnosis is confined to a combination of elevated peak PV velocity (≥ 110 cm/s) with turbulence and little flow variation (Fig. 7).48) In one study, TTE was also available for diagnosing PV stenosis before and after RFCA for AF.49) However, it is currently accepted that TTE or TEE are limited by its inability to image deeply into all four PVs and are less useful in establishing the extent and location of PV stenosis.50)
Go to :
Role of Transesophageal Echocardiography in AF
Identification and risk stratification of LA/LAA thrombus
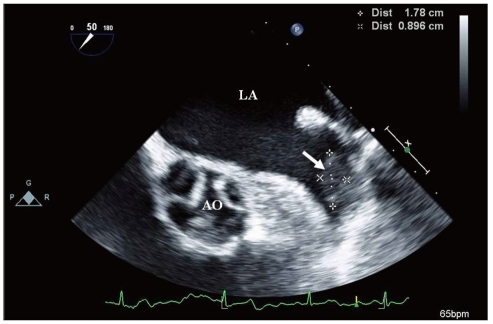
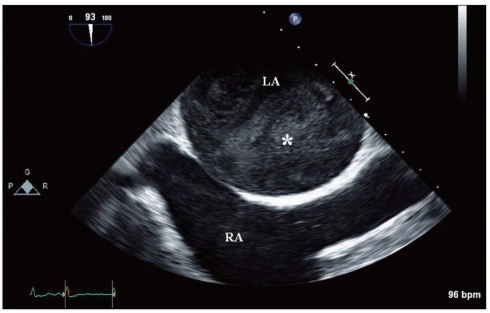
The risk of systemic emboli, probably arising in the LA cavity or LAA as a result of circulatory stasis, is an important consideration in AF. AF is considered to be responsible for almost half of all cardiogenic thromboembolism. One of the primary goals of management of patients with AF is the prevention of thromboembolic events. TTE has a low sensitivity for detection of thrombi in LA and especially LAA.51) TEE provides excellent visualization of posterior cardiac structures and is the modality of choice for detecting LA or LAA thrombi with a sensitivity and specificity of approximately 95% to 100% (Fig. 8).52) Thrombus identification is also challenging even if the appendage is visualized adequately. It is difficult to distinguish small thrombi from artifacts, including prominent trabecular structures, duplication artifacts, and adipose tissue within the transverse sinus. It is necessary to attempt to differentiate any suspicious abnormalities from thrombus in multiple views.
In the absence of formed thrombi, a dense SEC has been demonstrated to be a strong predictor of ischemic strokes (Fig. 9). When blood flow velocities are reduced in cardiac chambers and especially in the LAA, "smoke-like" echoes swirling in the cavity may be seen. An annual thromboembolic event rate of 12% has been observed in patients with SEC compared to 3% in patients without it.53) The finding of thrombus on TEE represents a poor outcome. In one study, it was associated with an embolic risk up to 10.4% per year and a death risk of 15.8% in a series of patients, most of whom were receiving anticoagulation therapy.54)
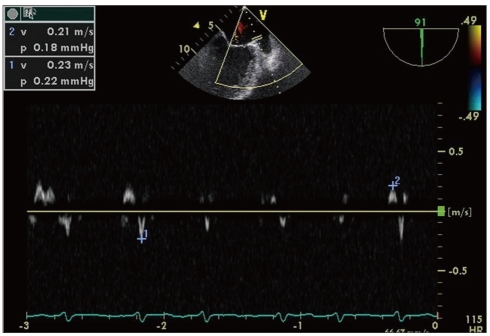
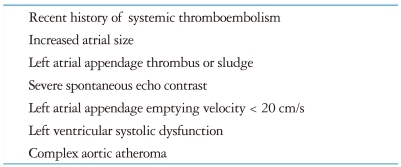
LAA was sometimes regarded as just a minor extension of the atrium. However, the importance of its function has been brought up because of its contribution to formation of thrombus. The mechanical function of LAA is best assessed with TEE utilizing pulsed wave Doppler measurement of LAA emptying and filling velocities (Fig. 10). In patients with sinus rhythm, LAA contracts once per cardiac cycle, and flow velocities at the ostium demonstrate a biphasic pattern with peak velocities generally exceeding 50 cm/s.55) Low LAA emptying flow velocities (< 20 cm/s) in AF correlate strongly with the presence of SEC and thrombus formation,56) whereas LAA emptying flow velocities > 40 cm/s predict greater likelihood to remain in sinus rhythm 1 year after successful cardioversion.53) For patients with AF, TEE risk factors of clinical thromboembolism include LAA thrombus, severe SEC, decreased (< 20 cm/s) flow velocities at LAA ostium, and complex aortic plaque (Table 1).56)57) A TEE performed 3 to 6 months after AF ablation can also evaluate thromboembolic risk and need for long-term anticoagulation, as echocardiographic risk factors may be present even if restoration of sinus rhythm is successful.
TEE-guided early cardioversion
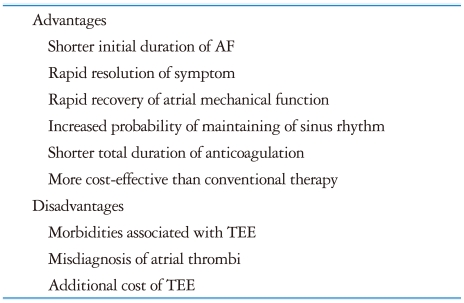
One of the primary goals of therapy in AF is the restoration and maintenance of sinus rhythm, with the aim of reducing symptoms and thromboembolic events. Cardioversion of AF to sinus rhythm can be performed with high rates of immediate success but unfortunately it may be complicated by embolic events in up to 7% of patients if the procedure is not preceded by several weeks of anticoagulation.61)62) Conventional care of patients with AF of prolonged (more than 48 hours) of unknown duration had required that these patients should be treated with oral anticoagulation for at least 7 weeks (3 weeks before and 4 weeks after cardioversion).63) The conventional approach to antithrombotic management before trying cardioversion has several potential disadvantages. This has promoted the recent suggestion of alternative approaches, such as TEE-guided early cardioversion. The advantages of TEE-guided early cardioversion with short term anticoagulation over the conventional strategy include the following: 1) In patients with no thrombus identified by TEE, the total duration of anticoagulation can be reduced by weeks, potentially reducing the risk of bleeding. 2) A shorter duration of AF before cardioversion is a strong predictor of AF recurrence following cardioversion. Therefore, early cardioversion with a TEE-guided approach might prevent the atrial remodeling and enable higher rates of sinus conversion and maintenance of sinus rhythm. 3) A TEE-based strategy could lower total costs by limiting laboratory tests, reducing preprocedural bleeding events, and improving clinical outcomes (Table 2).
However, thromboembolic events following cardioversion from AF were documented among patients with absent or subtherapeutic anticoagulation despite a negative TEE for thrombus,64) possibly caused by tiny thrombi that are undetected at TEE or as a result of new thrombus formation caused by LA/LAA stunning after cardioversion.24) Therefore, in current practice, TEE-guided early cardioversion includes screening for an existing thrombus and therapeutic anticoagulation at the time of TEE, as well as post-cardioversion anticoagulation prophylaxis to avoid new thrombus formation because of LA or LAA stunning (Fig. 11). The assessment of cardioversion using transesophageal echocardiography (ACUTE) multi-center randomized study demonstrated that embolic events and maintenance of sinus rhythm were similar in the two treatment strategies (conventional vs. TEE-guided early cardioversion), although the rate of hemorrhagic events was lower with the TEE-guided strategy.65) A new antithrombotic strategy of TEE-guided cardioversion with low molecular weight heparin has been suggested. The ACUTE II pilot study66) and randomized trial,67) which compared short-term antithbombotic therapy using low molecular weight heparin (LMWH) with intravenous unfractionated heparin (UFH), showed similar safety and efficacy with a lower length of hospitalization and more sinus rhythm in the LMWH group. In concert with precardioversion therapeutic anticoagulation with UFH, LMWH, or warfarin, TEE-guided early cardioversion is comparable to 4 weeks of precardioversion warfarin with a risk of clinical thromboembolism < 1%.65-67)
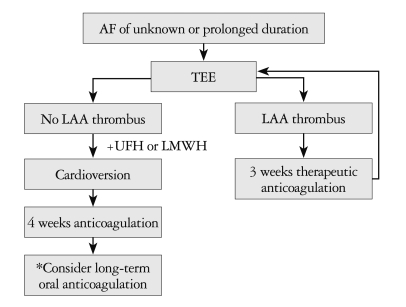 | Fig. 11Schematic flow chart of the transesophageal echocardiography-guided early cardioversion. *Long-term oral anticoagulation if stroke risk factors and/or risk of AF recurrence/presence of thrombus. AF: atrial fibrillation, LAA: left atrial appendage, UFH: unfractionated heparin, LMWH: low molecular weight heparin.
|
Go to :
Role of Intracardiac Echocardiography in AF
As mentioned above, RFCA with PV isolation has become as an effective therapy for patients with AF.68) ICE with 2D and Doppler technique is widely used in the practice of interventional electrophysiology. Advances in catheter-based ultrasound transducers and imaging technology provide more delicate images and enable direct visualization of anatomical structures when performing the RFCA procedures. This technique is quite safe with a negligible rate of complications and good patient tolerance. It allows improvement in success rate and decrease in complication when compared with fluoroscopic approach.69)
ICE enables the ready detection of some anatomical variations of LA such as PV and interatrial septal anatomy. Appreciation of these variations is essential to guide positioning of the circular mapping catheter and ablation catheter. Transseptal catheterization is an inevitable process of PV isolation. Anatomical variations of interatrial septum such as aneurismal septum, double membrane septum, patent foramen ovale, and others make this process complicated. ICE helps visualize the interatrial septum and detect some of the related anatomical variations that could be trouble during transseptal puncture. The use of ICE helps in determining the exact position of tip of the transseptal sheath by looking for tenting of the interatrial septum. The goal of transseptal puncture is to cross the septum in the posterior region of the fossa ovalis. It also enables avoidance of the life-threatening complication, such as perforation of lateral wall of LA or aortic root.
ICE allows for the adequate placement of the circular mapping catheter. Exact positioning and adequate contact of the catheter are very important, because they make delivery of radiofrequency (RF) energy effective and minimize the risk of complications, such as PV stenosis and thrombus formation.
ICE is useful as a monitoring tool for titration of energy power and/or duration. It can control lesion formation and prevent tissue overheating or structural perforation. Conventionally, temperature, power, and impedance are monitored during RF energy delivery. The appearance of microbubbles resulting from superheating can even precede increased impedance.70) Ablation needs to be terminated immediately if a sudden appearance of microbubbles is observed. This can prevent tissue damage and scar formation which may promote PV stenosis, LA perforation, or pericardial effusion.71)
ICE also allows early identification of complications related with procedure including damage to intracardiac structures, thrombus formation, PV stenosis, and pericardial effusion during RFCA.
ICE plays a valuable role during electrophysiologic procedures. Since it provides a lot of information about the intracardiac structures and hemodynamic assessments, ICE is expected to be used widely in clinical practice in the near future.
Go to :
Other Imaging Modalities in Management of AF
Other imaging modalities such as multidetector computed tomography (MDCT) and magnetic resonance imaging (MRI) provide more accurate measurement and better understanding of the cardiac anatomy, especially anatomical variations of PV and LA before RFCA of AF.72)73) MDCT and MRI have the additional advantage that it is operator-independent, unlike TTE, TTE, and ICE. As mentioned above, MDCT and MRI provide the best tests for evaluation of PV stenosis after RFCA of AF.50)
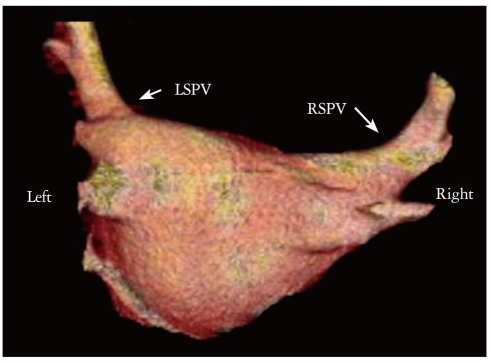
MDCT provides so high quality images of entire LA and each PV that these images are used with the electroanatomical mapping system to help guide the safe and effective RFCA of AF (Fig. 12).74)75) MDCT is increasingly being used to exclude thrombus and shows excellent negative predictive value.76) Another advantage of MDCT is that it enables to identify the extracardiac abnormalities, including pulmonary nodule, lung parenchymal disease, pleural abnormalities, hepatic problems, and others.77)
AF promotes atrial remodeling, resulting in the loss of atrial myocytes and increased collagen deposit and hence fibrosis of the LA wall.78) Delayed-enhancement MRI using gadolinium contrast is a novel noninvasive method to detect and evaluate the degree of remodeling or fibrosis associated with AF in the LA tissue.79) An increased amount of enhancement within the LA seems to be associated with AF recurrence after RFCA.79)
MDCT and MRI are promising tools for management of AF, however, radiation exposure and very high cost are the problem, respectively. Furthermore, it takes too long to examine and acquire images with these imaging modalities. Although clinical trials of pacemakers with new designs and protocols are underway, the risk of performing MRI in the presence of a permanent pacemaker or implantable cardioverter-defibrillator is still present in clinical fields. Therefore, adequate combination of the various imaging modalities allows for the proper management of patient with AF effectively.
Go to :
Conclusion
Because of the easy-accessibility, none or less-invasiveness, no radiation hazard, and few contraindications, both TTE and TEE are valuable tools that can provide cardiac anatomical and functional information. The advantages of echocardiography assist in the risk stratification, diagnosis of complications, and management of anticoagulation in patients with AF. The novel technique of ICE plays an important role during percutaneous interventional electrophysiology. MDCT and MRI have complementary role to echocardiography in the management of AF.
Ongoing advances in imaging acquisition and analysis in echocardiography will make the echocardiography more popular for evaluating and management of patients with AF.
Go to :
 XML Download
XML Download