

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Despite advances in medical interventions, infective endocarditis (IE) remains a disease entity with considerable morbidity and mortality.1-4) Poor prognoses of IE are related to valvular regurgitation and abscess formation secondary to tissue destruction, heart failure, and embolic complications.5) Risk factors of IE in industrialized countries are intravenous drug use, degenerative valve disease, intracardiac devices, health care-associated infection, and hemodialysis.4)6) Most cases of IE seemed to develop in patients with underlying structural heart disease. However, IE rarely involves the valves without predisposing abnormalities.
In Korea, Park et al.7) reported two cases about Streptococcus agalactias (S. agalactiae) IE with diabetes in 2006. In 2009, Lim et al.8) reported about the case of an S. agalactiae IE patient who also had advanced gastric cancer. On the contrary, we represent the case of a young, immunocompetent and non-pregnant woman patient who had structurally normal heart. There were major embolic event as the complication of S. agalactiae IE. Without any surgery, she made a complete neurological recovery after catheter directed thrombolysis. And The vegetation was disappeared after antimicrobial treatment without surgery.
Go to : 
Case
A 26-year-old woman who was previously healthy and had no history of chronic diseases was presented with sudden onset of mental change. Meticulous history taking revealed her history of dental scaling 6 weeks ago and intermittent fever for last 2 weeks. The patient did not have any obstetric and gynecologic problem such as recent abortion, and urine human chorionic gonadotropin (hCG) test was negative. When she had been transferred to our emergency department she showed confused mental status and fever of 38.5℃. The blood pressure was 110/70 mmHg and the pulse rate was 96 per minute. Grade III/VI systolic murmur was audible at the apical area. Physical examination revealed left eyeball deviation, complete gaze palsy with right hemiparesis (grade III/V), and global aphasia. Electrocardiogram showed sinus tachycardia. It was suspected that she had suffered from cerebroembolic events caused by IE. Emergent cerebral angiography was performed for the evaluation of suspected acute cerebral embolism. There was embolic obstruction at the distal portion of left internal carotid artery (ICA) (Fig. 1A). Catheter directed infusion by 200,000 unit of the urokinase was performed. Final angiography showed successful recanalization of ICA and middle cerebral artery (MCA) (Fig. 1B). Brain magnetic resonance imaging showed findings of acute infarction in left MCA territory and focal hemorrhage in left lentiform nucleus (Fig. 1C). Transthoracic echocardiography revealed a 0.8 × 0.5 cm-sized, highly mobile echogenic material on the posterior mitral valve (MV) leaflet suggesting vegetation (Fig. 2A). Three pairs of blood cultures were positive for S. agalactiae on admission. On the second day of antibiotic therapy, the bacterial cultures became negative. The patient was administered intravenous ceftriaxone for 4 weeks during the hospitalization. Follow-up echocardiography was performed on the seventh day of antibiotic therapy. It showed disappearance of the vegetation (Fig. 2B). There were no structurally abnormalities on MV (Fig. 2C). Only trivial mitral regurgitation was present after antibiotic therapy. She showed complete neurological recovery and got discharged.
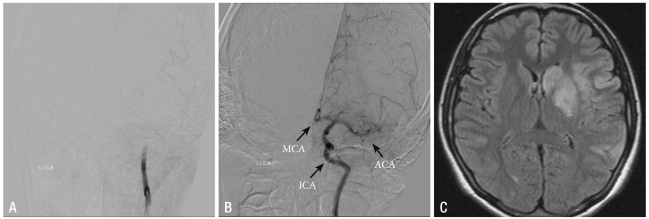 | Fig. 1Cerebral angiography shows complete thrombotic obstruction at the distal portion of left ICA (A). Final angiography after percutaneous thrombolysis shows good patency of left MCA, ACA and ICA (B). Brain MRI shows acute infarction in left MCA territory (circle) and focal hemorrhage in left lentiform nucleus (arrow) (C). ICA: internal carotid artery, MCA: middle cerebral artery, ACA: anterior cerebral artery, MRI: magnetic resonance imaging.
|
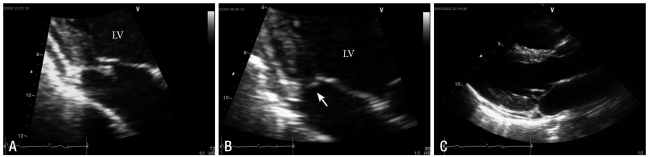 | Fig. 2Transthoracic echocardiography shows 0.8 × 0.5 cm-sized, echogenic and hypermobile mass on PMVL (A). Follow-up after antimicrobial therapy, echogenic mass was disappeared compared with previous study (B). Transthoracic echocardiography shows structurally normal MV during the end-systolic phase (C). PMVL: posterior mitral valve leaflet, MV: mitral valve.
|
Go to :
Discussion
IE features persistent bacteremia resulting from typical organisms for IE and evidence of cardiac valvular involvement (e.g. vegetation, new murmur of valvular regurgitation, paravalvular abscess).6) The incidence of IE is approximately 1.7-6.2 cases per year for every 100,000 patients. Despite advances in medical interventions, IE remains a disease with considerable morbidity and mortality.1-4)
In 2007, American Heart Association (AHA) revised the guidelines for IE prophylaxis to more clearly define when IE prophylaxis is recommended. They concluded that prophylaxis is reasonable only for patients with underlying cardiac conditions, for every dental procedures.9) IE has been well known for its occurrence in patients with underlying cardiac problems (e.g. rheumatic valvulopathies, congenital cyanotic heart diseases). However in recent other predisposing factors emerged, such as intravenous drug use, degenerative valve diseases, intracardiac devices, healthcare-associated infection, and hemodialysis. IE is now affecting patients without previously known valve diseases as the result of healthcare-associated procedures.
The mainstay of therapy of IE remains prompt antibiotic therapy. Surgery is indicated in specific patients of IE with congestive heart failure, perivalvular invasive diseases, fungal IE or uncontrolled infection despite maximal antimicrobial therapy.6)9)
Up to 65 percent of embolic events in IE involve the central nervous system, and neurologic complications develop in 20 to 40 percent of all patients of IE.5-7) The use of thrombolytic therapy in patients with IE suffering from embolic events is controversial. Whether the increased risk of intracranial hemorrhage in patients with IE is to be considered a contraindication for thrombolysis is unclear.
Traditionally S. agalactiae was an unusual pathogen in adults who are not pregnant.10) The incidence of invasive S. agalactiae infection was recently increasing in both elderly people and those with comorbid conditions.10)
In 2010, Ivanova Georgieva et al.11) underwent a cohort study about 27 IE patients due to S. agalactiae and reported that S. agalactiae IE often develops in patients who have underlying diseases such as diabetes mellitus, liver cirrhosis, malignancy, and abnormalities in immune responses. They suggested that S. agalactiae IE progress aggressively resulting in high mortality. Thus an urgent valve surgery should be performed where necessary such as the disease accompanies complications.11)12)
In our case, interestingly, the patient was a nonpregnant, immunocompetent and young woman who had no definite cardiac problems. Nevertheless, IE resulted in major stroke a life-threatening complication.
Decision making regarding the role of medical therapy or surgical intervention is complex and must be individualized to the patient. And it affects improvement of the prognosis in IE patients. In our case, we diagnosed IE with major stroke in early phase with echocardiography. And the patient was complete recovered neurologically by percutaneous intervention and prompt antimicrobial therapy without valve surgery.
Go to :
 XML Download
XML Download