

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Patent foramen ovale (PFO) is an increasingly recognized cause of cryptogenic stroke and peripheral embolism. Contrast transesophageal echocardiography (TEE) was established as a simple, accurate, and safe procedure for the diagnosis of interatrial communication. Paradoxical embolism is main pathophysiology via PFO, but this is mostly a presumptive diagnosis, while definite demonstration of a thrombus crossing a PFO is rare. Detection on thrombus-in-transit by echocardiography, the best management is controversy until now.
Case
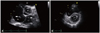
A previous healthy 53-year-old man was hospitalized with progressive dyspnea and cough for 2 weeks. Initial physical examination revealed a blood pressure of 126/81 mm Hg, respiratory rate of 20 per minute, and pulse rate of 103 per minute. On auscultation, heart sounds were tachycardiac and no murmur was heard. Examination of the lungs did not show significant pathological findings. The electrocardiography showed sinus tachycardia and inverted T wave on the anterior and inferior lead. Except for a plasma D-dimer level over 5,000 ng/mL (upper normal limit: 500 ng/mL), other laboratory findings were normal. Initial arterial oxygen pressure was 73 mm Hg, arterial carbon dioxide pressure 29 mm Hg, and oxygen saturation 94% at room air. Pulmonary computed tomography showed multiple filling defects of segmental branches of pulmonary arteries (Fig. 1). With the diagnosis of acute pulmonary embolism, intravenous heparin was started. In recalled previous history, he denied any predisposing conditions like as airplane travel or deep vein thrombosis.
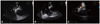
Transthoracic echocardiography (TTE) found wormlike, free-floating masses in the both atria (Fig. 2A). The right ventricle was moderately dilated (Fig. 2B) and mild tricuspid regurgitation was seen. Systolic pulmonary artery pressure was 80 mm Hg, and the inferior vena cava was dilated. No central pulmonary artery emboli or thrombi in the inferior vena cava were visible. Left ventricular ejection fraction was 61%. Right ventricular pressure overload resulted in D-shaped left ventricle and right ventricular systolic function was slightly depressed.
For further evaluation of mobile mass in the both atria, TEE was done. Interatrial septum was thin and mobile serpentine thrombi wedged through a PFO and lodged in both atria were demonstrated (Fig. 3A, Supplementary movie 1). Spontaneous cough during TEE, thrombi were disappeared (Fig. 3B, Supplementary movie 2) and color Doppler indicated right to left shunt (Fig. 3C, Supplementary movie 3). Immediately after TEE, oxygen saturation was decreased down to 84%, but with oxygen supplementation through a facial mask, it was elevated up to 95%. Neurologic examination was no abnormality of neurologic deficit. Due to a very high risk of paradoxical systemic embolism with potential disastrous consequences, he underwent emergent intravenous thrombolysis. Operation was not considered for his situation, because we couldn't trace the route of missing thrombus. The patient showed no clinical signs of paradoxical systemic embolism. Dyspnea was markedly relieved and follow-up chest computed tomography showed dissolved pulmonary thromboembolism. Follow-up echocardiography showed decrement of pulmonary artery systolic pressure 43 mm Hg. Further evaluation of hidden malignancy, all levels of tumor marker was normal range including carcinoembryonic antigen 1.4 ng/mL (normal 0-5 ng/mL), prostate-specific antigen 2.2 ng/mL (normal 0-3 ng/mL) and CA19-9 1.1 U/mL (normal 0-37 U/mL). Repeated chest computed tomography showed decreased size of multiple filling defects in both pulmonary arteries without evidence of lung cancer. Evaluation for hypercoagulable condition was not found any abnormal finding - protein C 82% (normal 70-140%), protein S 118% (normal 70-140%), and antithrombin III 94% (normal 80-120%). And serologic test for rheumatologic problem revealed normal range (anticardiolipin antibody: negative, lupus anticoagulant: negative). The patient was discharged from hospital with uneventful recovery and he has been doing well without additional embolic events after discharge and maintenance 24-month anticoagulation therapy.
Discussion
Paradoxical embolism was first described by Connheim in 1877 and is defined as the embolic entrance of venous thrombosis into the systemic circulation through a right to left intracardiac shunt, like as presence of PFO.1-3) This is mostly a presumptive diagnosis, while definite cases demonstrating a thrombus traversing the PFO are very few.4-6) A thrombus from the venous system into the right heart may easily cross into the left heart through a PFO if the right atrial pressure exceeds left atrial pressure, which can occur in the setting of pulmonary hypertension.2)4)6) Echocardiography, especially TEE, plays a main diagnostic tool in recognizing this potentially life-threatening, but treatable, condition.7)
Patients with a right-to-left intracardiac shunt via a PFO, agitated saline contrast-enhanced TEE is helpful. Interatrial pressure gradient can be reversed during cough or Valsalva maneuver. Cough test is known to be superior to Valsalva maneuver in the delineation of right to left shunt.8) Valsalva maneuver is contraindicated in patients with thrombus-in-transit via PFO - the risk of another embolism.
The best treatment for a pulmonary embolism with a thrombus straddled across PFO is unclear. Basically, the therapeutic options are cardiac surgery, thrombolysis, or anticoagulation with heparin, or a combination of all these treatments. Currently, surgical embolectomy and closure of PFO has been done as a preferred option.9-11) In our case, we decided the intravenous thrombolysis because of the patient's missing thrombus, although fragmentation of the thrombus followed by pulmonary or systemic embolization may be a theoretical risk of this treatment. Some previous reports described anticoagulant therapy can be used as an alternative treatment in this condition. 4)12)
We described a case of highly suspected paradoxical embolism with pulmonary embolism, in which a thrombus straddled and disappeared through PFO was observed in transesophageal echocardiography. In conclusion, thrombus-in-transit can be demonstrated by TEE in patients with pulmonary embolism and if detected, immediately treatment can prevent systemic embolism.

 XML Download
XML Download