

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The unicuspid aortic valve (UAV) is a very rare congenital heart disease that often requires cardiac surgery. The UAV shares many features with the bicuspid aortic valve. It is often confounded with bicuspid aortic valve, which is a more common congenital anomaly.
The estimated incidence of congenital UAV in the adult echocardiographic population was reported as about 0.02%. It was often discovered during surgery for aortic stenosis or post mortem.1) No case of UAV has been reported yet in Korea. We report the case of an asymptomatic patient presenting UAV with ascending aortic aneurysm, diagnosed by transthoracic echocardiography (TTE), transesophageal echocardiography (TEE), live three-dimensional (3-D) echocardiography, and 640-slice cardiac computed tomography (CT).
Go to : 
Case
A 50-year-old male was referred to our cardiovascular center for preoperative evaluation. He was scheduled to undergo cataract operation. Electrocardiography revealed voltage criteria for left ventricular hypertrophy. He was asymptomatic and physical examination revealed a systolic cardiac murmur on right upper sternal border. TTE showed noncalcified unicuspid aortic valve (Fig. 1), mild aortic stenosis (aortic valve area by planimetry = 1.64 cm2, mean pressure gradient = 14.6 mmHg), mild aortic regurgitation, and thickening at the basis of the left interventricular septum. An aneurysmal change of the ascending aorta reached a size of 5.27 cm. TEE revealed an eccentric valvular orifice, with rounded border on the leaflet of the free edge and a posterior single commissural attachment zone (Fig. 2). Live 3-D echocardiography confirmed the valve morphology (Fig. 3). Cardiac CT was planned to investigate possible coexisting cardiac anomalies, including an aortic aneurysm. CT demonstrated valvular morphology with dilatation of the ascending aorta with 6 cm in maximum diameter (Fig. 4) and no stenotic segment of the coronary arteries. He was offered additional surgery for the ascending aortic aneurysm and the UAV, but he refused it.
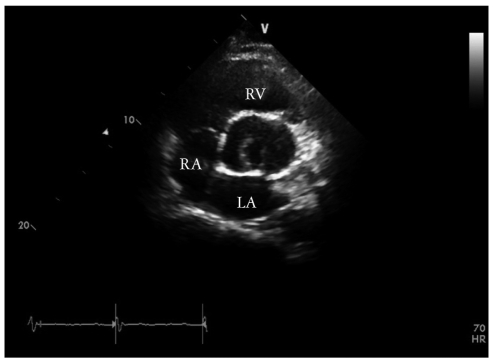 | Fig. 1Transthoracic echocardiography at the parasternal short axis view shows posteriorly situated eccentric aortic valve orifice extending to the annulus. LA: left atrium, RA: right atrium, RV: right ventricle.
|
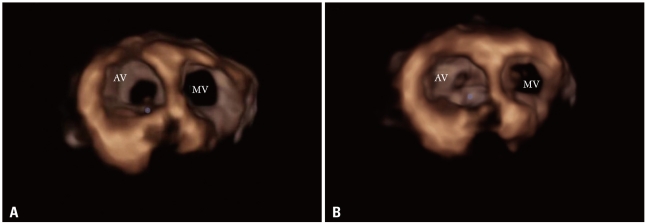
| Fig. 2Transesophageal echocardiographic mid-esophageal aortic short axis view (i.e. 50° view) is showing the unicuspid valve at systole (A) and diastole (B). A: In systole, the eccentric valvular orifice is extending to the annulus and showing a 'tear drop' opening. B: In diastole, there is posterior commissural attachment to the aorta. LA: left atrium, RA: right atrium, RV: right ventricle.
|

Go to :
Discussion
The UAV is a very rare congenital heart anomaly. During embryonic development, the aortic valve is formed from three tubercles, the fusion of which results in a UAV.2) The first report of the UAV was made by Edwards, in 1958.3) In one study by Cleveland Clinic, the estimated incidence was 0.02%.1) However, it was more frequent (up to 4-6 %) in patients undergoing surgery for pure aortic stenosis.4) The UAV was divided into 2 morphologic categories: one is the pin-hole shaped acommissural UAV, and the other is a slit-shaped unicommissural UAV.5) The acommissural UAV is usually accompanied by severe stenosis, therefore symptoms tend to be present at birth, and many patients undergo surgical intervention for severe stenosis during their infancy or childhood.6) The unicommissural form usually brings relatively larger orifice than acommissural form, thus it can be remained asymptomatic and hemodynamically stable until adulthood, which was the case in our patient. The UAV can be diagnosed by various imaging modalities, such as TTE, TEE, live 3-D echocardiography, cardiac CT, and/or magnetic resonanance imaging.7)8) The 3-D echocardiography helps to delineate the accurate anatomy of the aortic valve. It is a useful diagnostic method with potential advantages over the conventional 2-D echocardiography in the diagnosis of the UAV.9) In contrast, the cardiac CT can be considered as a complementary diagnostic tool because it clearly shows the great vessel anomalies, as well as the coronary arteries.10)
The UAV can also accompany with other cardiac anomalies, such as aortic regurgitation, aortic aneurysm, aortic dissection, patent ductus arteriosus, and the coarctation of aorta.11) The most common accompanying lesion is the isolated aortic stenosis.11) The ascending aortic aneurysm is known to be frequent in this condition, but information in the literature is limited to date.12) In the study conducted by Novaro et al.,1) the prevalence of ascending aortic dilatation was 48%. Agnihotri et al.12) reported significant aortic dilatation in 50% of their investigated patients. The aortic dilatation seemed to be caused by medial changes in the aortic tissue, which in turn may be related to embryogenesis.13) The aortic root dilatation of more than 50 mm should be considered as an indication for surgery to repair the aortic root or replace the ascending aorta, as in the bicuspid aortic valves.14)
We report a very rare case of UAV with ascending aortic aneurysm. The UAV with associated aortic aneurysm can be diagnosed by various diagnostic modalities. The optimal treatment strategies should be selected according to the clinical situation.
Go to :
 XML Download
XML Download