

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The left atrial (LA) calcification is a relatively uncommon complication of long-standing rheumatic valvular heart disease.1) Completed calcification of LA has been described as a 'coconut atrium'2)3) or 'porcelain atrium'.4)5) Porcelain atrium involves the LA appendage, the free wall of the LA and the mitral valve apparatus, except interatrial septum, whereas coconut atrium involves all areas of the LA.2-5) Porcelain atrium or coconut atrium is rare disease entity, furthermore the massive calcification of LA after mitral valve replacement has been reported very few the cases.6)7)
Authors experienced a 67-year-old woman who had massive LA calcification after mitral valve replacement. Therefore, we report this case with review of literature.
Case
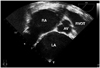
A 67-year-old woman was admitted to our hospital presenting with congestive heart failure (New York Heart Association functional class IV) and peripheral pitting edema. The patient had a history of mitral valve replacement for chronic rheumatic mitral valvular disease (severe mitral stenosis) in 1987 without evidence of LA calcification at the operation finding. An electrocardiogram showed atrial fibrillation and biventricular hypertrophy (Fig. 1). A chest X-ray revealed diffuse calcified outline of the left atrial wall and enlarged cardiac silhouette with cardiothoracic ratio of 82% (Fig. 2). Transthoracic echocardiogram showed a good motion of prosthetic mitral valve with increased mean diastolic pressure gradient about 6 mmHg and a mild mitral regurgitation. Three chamber enlargement except left ventricle with 87 mm-sized antero-posterior diameter of the LA (estimated volume index was 180 mm3/m2) and a severe tricuspid regurgitation were also shown. Transesophageal echocardiogram showed decreased LA contraction and increased spontaneous echo contrast in the LA chamber (Fig. 3). The estimated peak systolic pulmonary artery pressure was 70 mmHg and demonstrated severe pulmonary hypertension. Chest computed tomogram showed massive calcification of the LA (Fig. 4). The surgery was performed for right heart failure in February 2008. We performed tricuspid valve annuloplasty with annular ring (33 mm-sized Tailor® Flexible Ring, St. Jude Medical, St. Paul, MN, USA) and removal of subvalvular structure with myotomy and endoatriectomy of right atrium under cardiac arrest with a cardiopulmonary bypass. The patient's symptom was improved after the surgery and discharged without any complications.
Discussion
The first presentation of LA calcification was made by Oppenheimer8) in 1912. He first described the post-mortem findings on a 44-year-old male who died of congestive heart failure due to mitral stenosis. Harthorne et al.9) reviewed 16 cases of LA calcification in 1966. Massive calcification of the LA was predominant in woman as frequent as 74% and was usually associated with rheumatic mitral stenosis. It took an average duration of 19.7 years to diagnose massive LA calcification after rheumatic mitral stenosis.9) However, massive calcification throughout the LA wall is very rare.
The pathophysiology of the LA calcification associated with mitral valvular disease were 1) a previous ulceration of the atrial wall as the origin of the calcification and 2) a response to the chronic strain forces in the setting of mitral disease.1) It is also rarely reported in chronic renal failure.10-12) Massive calcification of the LA wall can cause recurrent thrombosis despite the therapeutic anticoagulant level of the patient following a surgical thrombectomy.13) Roberts et al.14) reported that calcific deposits prevented the LA from dilating, decreased its compliance, and caused the elevated LA pressure to be transmitted to the pulmonary vessels and the right ventricle, leading to tricuspid insufficiency. In our case, LA calcification was progressed after mitral valve replacement despite there was no definite LA wall calcification at the time of surgery. We thought it was due to previous formed rheumatic ulceration of the atrial wall as the origin of the calcification and its progression.
Radiography of the left side of the chest is recommended to assess long-standing rheumatic mitral valve disease. The image of computed tomography can display massive atrial calcification rather than the plane chest X-ray. In general, transesophageal echocardiography permits admirable visualization of the LA compared with transthoracic echocardiography because of the anatomic accessibility of the esophagus. However transesophageal imaging is significantly impaired in the presence of calcified walls of LA.15) Adequacy of transesophageal and transthoracic echocardiographic imaging possibly depends on the extent and the density of calcification.16) Magnetic resonance imaging may demonstrate the presence of thrombus, but its ability to depict the atrial calcification is suboptimal.3)
Surgery should be considered as one option of the treatment for atrial calcification.1) But no postoperative investigation has been done to evaluate the long-term mortality and the progression of the atrial compliance after the operation.
In conclusion, in patient with long lasting rheumatic valvular heart disease it is possible that progression of LA calcification after mitral valve replacement despite there was no LA wall calcification at the time of surgery. Thus, if patient who had rheumatic heart disease and underwent mitral valve replacement, suffer right heart failure, extensive LA calcification should be considered.



 XML Download
XML Download