

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Blood-filled cysts of the heart have been reported in infants by necropsy, but are rare in older children and adults. Blood-filled cysts were usually found on the valvular endocardium and thought to have no clinical significance in previous reports. The optimal management of asymptomatic blood-filled cyst is not determined. We experienced an adult case of a blood-filled cyst on the top of anterolateral papillary muscle, which was successfully removed without valvular damage.
Case
A 22-year-old man visited out-patient clinic for the evaluation and treatment of cardiac mass. The mass was found incidentally during the work up for intermittent chest pain at a secondary referral hospital. Physical examinations revealed blood pressure of 102/64 mmHg, a heart rate of 80 bpm, and a respiratory rate of 20 breaths/min. There were no thrills, murmur or abnormal sound on cardiac examination. Laboratory findings showed normal blood chemistry, blood count, liver function tests and coagulation profiles. An electrocardiogram revealed normal sinus rhythm and a chest radiography showed unremarkable finding on admission.
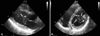
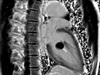
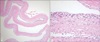
The transthoracic echocardiography showed 1.6×2.1 cm-sized ovoid mass attached to the head of anterolateral papillary muscle (Fig. 1). The surface of the mass had a partially high-echoic density, and inside of the tumor appeared echolucent or echo-free, which was clearly distinguished from myocardial echodensity. The mass did not cause valvular dysfunction or diastolic flow disturbance. The same findings were observed on transesophageal echocardiography. On cardiac MRI, this mass showed iso-signal intensity on T1-weighted image and high signal intensity on T2-weighted image. After gadolinium administration, the delayed image showed no enhancement in the mass (Fig. 2). On the operation field, a blood-filled cystic mass attached to the top of anterolateral papillary muscle was found. This mass was excised and chordae reinforcement was done by using da Vinci system. This operation did not cause any damage on the mitral valve. Histological examination revealed that the cyst consisted of thick fibrous wall and endothelial lining, and subendothelial aggregation of blast-like cells with multi-lineage differentiation (Fig. 3). The patient showed uneventful recovery after surgery.
Discussion
Blood-filled cysts on the heart valves were first reported by Elasser in 1844. In autopsy series of 112 cases of fetal and infant hearts, blood-filled cyst was present in 56%, which suggested that it would not be rare in infants.1) However, it is extremely rare in the adult. Histologically, these cysts are composed of endothelial cell lining and fibrous tissue.
Several theories have been suggested about the origin of blood-filled cyst. Boyd2) and Kantelip et al.3) suggested that the cysts give rise during the cardiac structural development. These theories implied congenital development of blood-filled cyst. On the other hand, some investigators have proposed that sudden occlusion of vessels due to certain factors such as inflammation, vagal stimulation, anoxia, and coagulation disorders lead to hematoma formation.4) Another hypothesis is that blood cysts may be derived from ectatic blood vessels or angiomas.5)
In this case, echocardiography was an excellent modality for identifying intracardiac mass and effect of this mass on valvular function. Blood-filled cyst has typical echocardiographic findings of smooth outer surface and echolucent cavity like this case. Cardiac MRI also could be valuable to differentiate blood-filled cyst from other masses. On precontrast examinations, blood-filled cysts are isointense compared to myocardium on T1-weighted images and hyperintense on T2-weighted images like hemangioma cases.6) However, on the contrary of hemangioma,7) blood-filled cysts do not show delayed filling in the late phase of contrast administration.
Blood-filled cysts have been reported to develop on the valvular apparatus or papillary muscle of the tricuspid, pulmonary or mitral valves. Several cases of blood-filled cysts attached to the papillary muscle were reported.8-11) Hauser et al. reported a blood-filled cyst attached to the tip of the anterolateral papillary muscle of the mitral valve in a 27 year-old man with an embolic event.8) The cyst was removed with a replacement of the mitral valve. Arnold et al.9) also reported a blood-filled cyst attached to the papillary muscle which caused left ventricular outflow tract obstruction. Excision of cyst and valve replacement were performed in this patient. In our case, the patient had no specific symptom except intermittent chest pain and no valvular dysfunction. Although there are no consensus on the surgical indication of a blood-filled cyst without causing valvular dysfunction or flow obstruction, a surgical removal without valve replacement was performed in our patient to prevent embolic risk and rule out malignant pathologic conditions.
 XML Download
XML Download