

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Primary cardiac neoplasms are very rare, with an incidence less than 0.2% in unselected patients at autopsy.1) Of these, cardiac myxomas are the most common benign cardiac tumors.2) Although cardiac myxomas are histologically benign, they tend to form emboli and cause intracardiac obstruction. So they should be classified as potentially fatal tumors. Tumoral embolism is the second common clinical presentation of myxomas and can affect systemic and/or pulmonary circulation, depending on the tumor's location and the foramen ovale's patency.
Though acute myocardial infarction (AMI) can be caused by coronary myxoemboli, it is very rare and can be the first clinical presentation of left cardiac myxoma. In patients with acute ST elevation myocardial infarction (STEMI), rapid recanalization of coronary arteries is the most important factor determining clinical prognosis. However, in many cases of AMI caused by cardiac myxoma, open heart surgery and excision of the coronary artery have been the best treatment options to remove the myxoma and embolus from the coronary artery to maintain distal coronary flow.3) In cases of STEMI, however, preparing for emergent open heart surgery takes a considerable amount of time and can worsen the coronary perfusion to the infarcted area. Recently, the Export aspiration catheter (Medtronic, Minneapolis, Minnesota), a 6Fr aspiration system with a 20 cc syringe, has been introduced to the intervening fields. With this catheter we can remove a thrombus manually from an infarcted coronary artery.
In this case report we present a case of acute anterior STEMI caused by left atrial villous myxoma. The patient was successfully treated with intracoronary catheter aspiration to maintain distal coronary flow.
Case
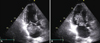
A 65-year-old woman with hypertension was admitted to our emergency room for acute chest pain and dysarthria. On her arrival, her blood pressure was 170/92 mmHg, her pulse was 86 beats per minute, her axillary temperature was 36.3℃ and her respirations were 20 breaths per minute. She had a tumoral plop and diastolic cardiac murmurs. Blood analysis showed erythrocyte sedimentation rate/C-reactive protein (ESR/CRP), creatine kinase MB (CK-MB) and troponin I within the normal range. A radiograph of her chest showed pulmonary vascular prominence without edema or infiltration. An electrocardiogram revealed ST-segment elevation in leads V1-V5. Transthoracic echocardiogram showed mild left ventricular systolic dysfunction with akinesis of the left ventricle's anterior, septal and apical walls, suggesting infarction of the left anterior descending coronary artery (LAD). A mass in the left atrium was attached to the atrial septum. This mass demonstrated high mobility and a villous nature, and was about 2.5 cm wide by 9 cm long (Fig. 1). Magnetic resonance imaging of her brain showed new-onset multifocal cerebral infarction foci.
Primary percutaneous coronary intervention (PCI), performed approximately two hours after her symptoms' onset, revealed a total occlusion in the distal LAD (Fig. 2A). The lesion was treated with intracoronary suction aspiration by an Export aspiration catheter and a small embolus was removed. After the aspiration, the distal LAD was fully reperfused (Fig. 2B).
The patient underwent open heart surgery to remove the left atrial myxoma. Its pathology was compatible with a villous myxoma. After resection, she was discharged with no complications.
Discussion
Cardiac myxomas are the most common primary benign cardiac tumors with an increased risk of systemic embolization. The probability of arterial embolism is closely related to the tumor's morphology, and villous myxomas are more fragile, and form embolisms more often, than other tumors.1)4) The reported embolic events' rates are about 45-60% for myxomas of the left heart and about 8-10% for right heart myxomas.5)
Though coronary arteries can be occluded by the emboli from myxoma, this event's reported incidence is very low. This low incidence of coronary embolism likely arises from the right angled junction of the coronary apertures within the aortic bulb, the aortic valve cusps' protection of the coronaries and the coronary apertures' small diameter. However, villous myxomas form emboli as a result of their tendency to fragment, often resulting in small tumoral particles that can pass through the coronary apertures.6)
AMI is a major cause of mortality and morbidity worldwide. Although most cases of acute STEMIs result from ruptures of vulnerable coronary atherosclerotic plaques with superimposed coronary thromboses, they also can occur in normal coronary arteries. STEMIs' prevalence in normal coronary arteries has been reported as 1-7% in various angiographic, intravascular ultrasound (IVUS) and autopsy studies.7) Numerous pathological processes other than coronary atherosclerosis include emboli to coronary arteries, usually from myxomas, congenital coronary arterial anomalies, myocardial oxygen demand-supply disproportion, and hematological and miscellaneous causes.8)9)
Management of acute STEMI includes rapidly restoring epicardial coronary blood flow by pharmacological and catheter-based approaches, antithrombotic therapies to suppress recurrent ischemic events, and treatments to decrease myocardial necrosis and prevent future events.10) Rapid recanalization with primary percutaneous coronary intervention shows better clinical results than thrombolytic therapy.11)
Open-heart surgery and excision of the coronary embolus have been one of the options for treating acute STEMI from an embolism.3) Adjunctive thrombectomy with an aspiration catheter can give physicians an opportunity to remove the coronary thrombus and offers microvascular protection during primary PCI.12) Unfortunately, no reported patient has undergone removal of an embolus in an infarcted coronary artery in a primary PCI setting.
In this report, we present a case of acute anterior STEMI caused by a left atrial villous myxoma. The patient was successfully treated with intracoronary catheter aspiration to restore distal coronary flow. Thus, we suggest that the intracoronary catheter aspiration can be an adequate option in patients with acute myocardial infarction caused by a left atrial myxoma.

 XML Download
XML Download