

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Apical hypertrophic cardiomyopathy is a variant of hypertrophic cardiomyopathy (HCM) characterized by a spade-shape configuration on echocardiographic examination. It often accompanies a quite normal or even larger coronary arteriogram. Therefore acute myocardial infarction with significant atherosclerosis is rarely reported in patients with apical HCM or hypertrophic cardiomyopathy. Also there was no report of apical HCM combined with acute myocardial infarction and multiple coronary thrombosis. We report a rare case of typical apical HCM, who developed acute myocardial infarction due to multiple coronary thrombosis.
Case
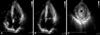
47-year-old man was admitted to Eulji University Hospital due to chest pain of sudden onset after swimming. One year ago, he was already diagnosed as having apical HCM. He had neither history of hypertension, diabetes nor smoking. On physical examination, blood pressure was 114/70 mmHg, pulse rate 70/min, and respiratory rate 15/min. On auscultation of chest, S1 and S2 sound were normal without heart murmur. Laboratory studies revealed total cholesterol of 174 mg/dL, triglyceride of 42 mg/dL, HDL-cholesterol of 68 mg/dL, glucose of 96 mg/dL, and uric acid of 8.1 mg/dL. The electrocardiogram showed regular sinus rhythm with ST elevations in the lateral leads and ST depression in anterior chest leads (Fig. 1). On cardiac enzyme test, CK-MB and troponin-T level were markedly elevated. The trans-thoracic echocadiography revealed the typical spade-shaped configuration and with a marked increment in apical wall thickness. On the apical four chamber view, anteriorseptal and apical wall were hypokinetic in motion (Fig. 2). The Doppler echocardiography showed diastolic dysfunction, moderate in degree and without LV outflow tract dynamic obstruction. Based on coronary arteriogram, the distal left anterior descending, its diagonal branch, left circumflex and its obtuse marginal branch coronary arteries were found to be totally cut off with thrombi. In addition, coronary artery flow was slow with opacification of the arteries significantly delayed in the absence of significant epicadial coronary disease (Fig. 3). Then abciximab and heparin were intravenously infused in concert with temporary pacemaker insertion. Percutaneous coronary angioplasty on first diagonal branch of the left anterior descending artery with 2.5 mm balloon was tried, but without success. Obstuse marginal branch of the left circumflex artery was successfully treated with suction catheter. Obstruction of the left anterior descending artery had come to a settlement by intracoronary administration of urokinase 200,000 units. Two days later, coronary blood flow was restored on follow-up coronary angiography.
Discussion
HCM is characterized by a thickened but nondilated LV in the absence of another cardiac or systemic condition that can produce LV hypertrophy.1) Segmental wall thickening mostly confined to the distal portion of LV chamber, is a distinctive feature of apical HCM, which is often concomittently associated with a spade shape of the LV chamber and marked T wave inversion on the electrocardiogram.2) Genetic relationship between HCM with typical hypertrophic morphology versus apical HCM is incompletely understood.3) The clinical course of apical HCM is varies, however most HCM patents may remain stable over long periods of time; up to 25 percent of a hospital-based HCM cohort was reported achieve normal life span with little or no disability, and without the necessity for major therapeutic intervention.1)4) At variance with this usual expectation, our patient admitted to emergency room due to acute myocardial infarction. The coronary arteriogram revealed the complete obstruction of both the distal left anterior descending coronary artery with its diagonal branch and the left circumflex coronary artery with its obtuse marginal branch. Despite intravenous infusion of abciximab and unfractionated heparin along with temporary pacemaker insertion and percutaneous coronary intervention, epicardial coronary blood flow was not improved. We incorporated recent advances in background medical therapy, i.e. abciximab use at the time of percutaneous coronary intervention procedures, which may partially explain the lower than expected event rate in acute myocardial infarction.5)
There was no report of apical HCM combined with acute myocardial infarction and multiple coronary thrombosis. Although various hypotheses have been proposed that explain the mechanism of myocardial infarction without significant epicardial coronary atherosclerosis, the true mechanism has yet to be elucidated. Increased myocardial mass, intramyocardial small vessel disease, inadequate vasodilator reserve, septal perforator artery compression, coronary artery spasm, elevated filling pressures related to impaired diastolic relaxation and increased oxygen demand due to dynamic LV outflow gradients have all been suggested as plausible mechanisms of myocardial ischemia.6)8) Although we could not find specific causes of multiple coronary thrombosis, it was definite that this patient had no systemic disease that can create thromboembolic phenomenon. In this respect, we assumed that slow coronary artery flow is the most possible clinical scenario that can account for multiple coronary thrombosis. Slow coronary artery flow caused coronary artery thrombus, and then the thrombus may have subsequently led to acute myocardial infarction. This presumption was further supported by delayed distal vessel opacification in the absence of significant epicardial coronary disease, which is believed to represent coronary microvascular dysfunction.7)8) Hahm et al. have already reported on a case of HCM with myocardial infarction and a normal coronary arteriogram, this is the first documented combination of slow coronary artery flow and HCM in Korea.9) The pathologic reports make intramural coronary artery disease the most likely mechanism that induces acute myocardial infarction in patients with HCM. Maron et al. described the clinical and morphologic features of seven patients who suffered from both HCM and transmural myocardial infarction without significant atherosclerotic narrowing of the extramural coronary arteries.10)
In summary, we present a rare case of apical HCM, who developed acute myocardial infarction due to multiple coronary thrombosis.


 XML Download
XML Download