

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Double-orifice mitral valve (DOMV) is a rare congenital malformation. This anomaly is usually detected at an early age because it is frequently associated with other cardiac malformations. However, there also have been a few reports of isolated DOMV. In these patients, the mitral valve function is usually normal, and most of the patients are asymptomatic at the time of diagnosis. We experienced a case of mitral valve prolapse and severe regurgitation of congenital DOMV.
Case
A 27-year-old woman visited out-patient clinic for the treatment of mitral regurgitation. She was told about 7 years ago that her mitral valve was abnormal. Severe exertional dyspnea (NYHA functional class III) and orthopnea were developed 1 month ago. She underwent cardiac evaluation at a university hospital and referred to Asan Medical Center for further evaluation and cardiac surgery. On the physical examination, a harsh pansystolic murmur grade 5/6 was heard at the apex.
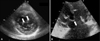
Transthoracic echocardiography showed dilated left atrium and left ventricle with normal ejection fraction. Mitral valve was divided into 2 separate valve orifices (anterolateral & posteromedial) by a fibrous bridge (Fig. 1). On the apical 2 chamber view, center part of anterior mitral leaflet, fibrous bridge did not move toward apex at diastole while the medial and lateral parts did, which looked like wings of flying seagull. The color Doppler image showed 2 separate mitral inflows through 2 separate orifices at diastole on the apical 2 chamber view. The lateral scallop of the posterior mitral valve leaflet (P1 segment) prolapsed into left atrium at systole and severe eccentric mitral regurgitation jet toward medial side was observed. The same findings were observed on transesophageal echocardiography and no ruptured chordae was shown (Fig. 2). No other congenital cardiac anomaly was detected. In the operating room, congenital DOMV with balanced size of 2 orifices accompanied with severe P1 segment prolapse without ruptured chordae was seen (Fig. 3). Mitral valve was successfully repaired with lateral commissural repair and ring annuloplasty (cosgrove 32) using da Vinci system.
Discussion
DOMV is a rare disorder that was first reported by Greenfield in 1876.1) Rosenberg et al. stated that the true developmental basis of duplication of the mitral valve is unknown.2) Bano-Rodrigo et al., however, proposed that the DOMV is the result of an early arrest of development and that the accessory orifice represents a retention of the left portion of the common atrioventricular canal with subsequent reduction of the mitral ostium and alignment with it.3)
DOMV can be seen either as an isolated malformation or in association with other cardiac anomalies. According to a previous report, atrioventricular septal defect was the most commonly associated lesion (52%), followed by obstructive left-sided lesions (41%), and cyanotic heat disease (11%).4) In our case, no other congenital cardiac anomaly was detected.
The classification based on echocardiographic imaging was proposed by Trowitsch et al, which divided DOMV into 3 different types: 1) hole type (accessory orifice surrounded by leaflet tissue that may have a chordal ring), 2) complete bridging (fibrous bridge in the plane of the mitral valve sails, dividing the mitral valve opening into 2 parts that may be equal or unequal), and 3) incomplete bridging (small strand of fibrous tissue connects only the tips of the anterior and posterior leaflets).5) Complete bridging type as our case is reportedly most common, where 2 distinct orifices are seen in all levels of mitral valve leaflets.
Although hemodynamic disturbance is not observed in most cases of DOMV, significant mitral regurgitation and/or stenosis are associated in some patients. Bibhuti et al. reported that the mitral valve was functionally normal in 9 patients (50%) and only mildly impaired in 7 (38%), and that only 2 patients (11%) had severe mitral regurgitation or stenosis.6) In our case, severe mitral regurgitation due to severe P1 prolapse without ruptured chordae was observed. The mitral valve was successfully repaired with lateral commissural repair and ring annuloplasty using da Vinci system. In 4 previous reports about DOMV accompanied with severe mitral regurgitation, mitral valve was successfully repaired or replaced.7-10) According to Bano-Rodrigo et al, fibrous bridges between 2 orifices should not be transected surgically, because these bridges are composed of mitral leaflet tissue and chordae which are essential to maintain valve integrity.3)


 XML Download
XML Download