

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Endoscopic retrograde cholangiopancreatography (ERCP) is difficult to perform in patients with a Billroth II gastrectomy because of anatomical changes. The success rate of ERCP and endoscopic sphincterotomy in patients with a Billroth II gastrectomy is lower than that in patients with normal anatomy. In our case, a 76-year-old man with altered anatomy after a Billroth II gastrectomy underwent cap-assisted forward-viewing endoscopic cholangiopancreatography because of bile duct stones. We successfully performed a fistulotomy followed by large-diameter balloon dilation of the fistulotomy tract for the management of choledocholithiasis in this patient with a history of a Billroth II gastrectomy.
Figures and Tables
Fig. 1
Abdominal CT scan. It demonstrates dilated intrahepatic bile duct and a 17×13 mm sized CBD stone in the distal CBD.
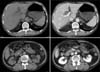
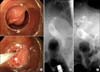
Fig. 2
Fistulotomy in a Billroth II patient. (A) The duodenal base of the papilla was pushed with the 11-o'clock margin of the cap, the papilla was turned to face the endoscope. After needle puncture of the bile duct, a soft-tipped 0.025 inch guidewire was advanced to gain access to the CBD after the fistulotomy. (B) After deep cannulation with the guidewire was achieved, cholangiogram was attained. Cholangiogram showed a 17×13 mm sized filling defect in the dilated CBD. (C) Two plastic stents were deployed into the CBD.

References
1. Faylona JM, Qadir A, Chan AC, Lau JY, Chung SC. Small-bowel perforations related to endoscopic retrograde cholangiopancreatography (ERCP) in patients with Billroth II gastrectomy. Endoscopy. 1999. 31:546–549.

2. Lin LF, Siauw CP, Ho KS, Tung JC. ERCP in post-Billroth II gastrectomy patients: emphasis on technique. Am J Gastroenterol. 1999. 94:144–148.
3. Forbes A, Cotton PB. ERCP and sphincterotomy after Billroth II gastrectomy. Gut. 1984. 25:971–974.
4. Osnes M, Rosseland AR, Aabakken L. Endoscopic retrograde cholangiography and endoscopic papillotomy in patients with a previous Billroth-II resection. Gut. 1986. 27:1193–1198.
5. Park CH, Lee WS, Joo YE, Kim HS, Choi SK, Rew JS. Cap-assisted ERCP in patients with a Billroth II gastrectomy. Gastrointest Endosc. 2007. 66:612–615.
6. de Weerth A, Seitz U, Zhong Y, Groth S, Omar S, Papageorgiou C, et al. Primary precutting versus conventional over-the-wire sphincterotomy for bile duct access: a prospective randomized study. Endoscopy. 2006. 38:1235–1240.
7. Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, Dorsher PJ, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996. 335:909–918.
8. Mavrogiannis C, Liatsos C, Romanos A, Petoumenos C, Nakos A, Karvountzis G. Needle-knife fistulotomy versus needle-knife precut papillotomy for the treatment of common bile duct stones. Gastrointest Endosc. 1999. 50:334–339.
9. Ersoz G, Tekesin O, Ozutemiz AO, Gunsar F. Biliary sphincterotomy plus dilation with a large balloon for bile duct stones that are difficult to extract. Gastrointest Endosc. 2003. 57:156–159.
10. Jun DW, Choi HS, Park SH, Lee HL, Lee OY, Yoon BC, et al. A role of endoscopic balloon dilatation after partial infundibulotomy in billroth II patients. Korean J Gastrointest Endosc. 2007. 35:74–79.
 XML Download
XML Download