

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
In the urinary tract, sarcomatoid carcinoma is a very rare malignant neoplasm. The tumor consists of carcinomatous tissues originating from epithelium cells and multiform cells originating from the mesenchymal components of either poorly differentiated or spindle cells. The tumor cells have specific characteristics that indicate that they are mixed within their own border. Sarcomatoid carcinoma is known to occur in only 0.3% of total bladder cancers;1 according to domestic reports (Korea), one case was reported as a sarcomatoid carcinoma confined in the bladder, and other cases included sarcomatoid carcinomas confined in the pelvis of the kidney or in the diverticulum in the bladder.2 Sarcomatoid carcinomas are typically malignant with a very fast growth velocity, such that once diagnosed, most cases have a poor prognosis because the patients have already advanced to a stage at which the carcinoma has already invaded the surrounding tissues. The purpose of this report is to present a case of sarcomatoid carcinoma in the bladder, in which a 78-year-old male patient was diagnosed with a painless gross hematuria that developed in the right lateral wall of the bladder. We also review the related literature.
Case Report
A 78-year-old male patient had a history that included painless, severe gross hematuria that began 2 weeks before his diagnosis. He was thus referred to our hospital on the basis of a kidney and bladder ultrasound that was performed at a local clinic. During the initial evaluation at the clinic, a 2.5×1.6 cm irregular hyperechoic mass was found on the right lateral bladder wall, and the patient was therefore referred to our institution.
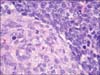
No specific symptoms or signs were noted in the initial review of systems or in the physical examination, with the exception of the severe gross hematuria, and the patient did not have a specific past surgical or medical history. His serum creatinine, Hb, and platelet values were 1.4 mg/dl, 9.2 g/dl, and 94,000/ml, respectively, with 10~19 RBC/HPF and 20~29 WBC/HPF obtained from a urine analysis. Other laboratory examinations all fell within the normal range. The gross hematuria continued, and as a result, the patient's blood pressure decreased to 80/50 mmHg. Emergency TURBT was then performed under the impression that the patient had bladder cancer. A cystoscopic examination revealed a broad-based tumor 4 cm in diameter on the lateral side of the right ureteral orifice. The mass was revealed to be a non-papillary, large, bulky tumor having a necrotic tumor surface. Despite several attempts, we could not perform a complete resection because of the danger of bladder perforation. As such, we subsequently controlled the bleeding and finished the surgery. Microscopically, the sizes of the cancer cells were relatively uniform and dense. The shape of these cells generally looked like whirlpools in a pyramid-shaped bundle, although some cells were composed of epithelioid cells or irregular-shaped multiform cells. Under high magnification, a minimum of 3 mitosis periods were observed and the cancer was considered malignant (Fig. 1). A subsequent immunohistochemical examination showed that the area of the epithelium component was positive for cytokeratin, one of the characteristics of carcinoma; also, the nonepithelial area tested positive for vimentin, an indicator of sarcoma. Therefore, we determined that the cancer was a sarcomatoid carcinoma (Fig. 2). During the stage work-up after the operation, an abdomen-pelvic computed tomography scan showed a remnant 4.0×1.5 cm-sized hypervascular mass on the right lateral wall of the bladder and multiple lymph node metastases (Fig. 3). In addition, the whole-body bone scan showed multiple bone metastases. The patient had gross hematuria, making voiding difficult, and displayed general weakness only 2 months after surgery. Based on these symptoms, he visited the hospital as an outpatient, and with his family made arrangements for home hospice care. He expired 1 month after initiating home care.
Discussion
Sarcomatoid carcinoma of the urinary bladder is a very rare tumor. Although more than 70 cases of primary sarcomatoid carcinoma of the urinary bladder have been reported in the literature,3 only 1 case has been previously reported in Korea.2,4 This tumor contains both the sarcoma element from mesenchymal tumors and the carcinoma element from epithelial cells. The mesenchymal component may be expressed as a variety of histologic types, including chondrosarcoma, leiomyosarcoma, osteogenic sarcoma, and rhabdomyosarcoma. The epithelial component may be most frequently found in transitional cell carcinoma, adenocarcinoma, or in an admixture of these. As such, the tumor has been previously described under a variety of names, such as sarcomatoid carcinoma, pseudosarcoma, malignant mixed mesodermal/Mullerian tumor, metaplastic carcinoma, and spindle cell carcinoma.2 Sarcomatoid carcinoma is a cancer that has the appearance of the prominent spindle cells and in most cases occurs in the uterus, although it also occurs in the breasts, ovaries, urinary system, oral cavity, and esophagus.4-7 The carcinosarcoma is classified as a mosaic condition of totally different epithelial cell elements and sarcomatoid cell elements; if the carcinosarcoma has characteristics of dysmorphic differentiation into the cartilage and skeletal muscle, it can be considered a carcinosarcoma. However, carcinomatous sarcoma and sarcomatoid carcinoma have similar clinical courses, and no histological or clinical differences have been shown between these two classifications of cancer. Hence, the clinical usefulness of separating carcinosarcoma from sarcomatoid sarcoma (carcinoma with spindle cell carcinoma component) is uncertain. This tumor predominantly occurs in male smokers; the male:female ratio is approximately 3:1 with a mean onset age of 72 years (49 to 88),8 and the most common presenting symptom is gross hematuria, similar to that in transitional cell carcinomas.9 The predominant location of carcinosarcomas is the bladder base, followed by the trigone and lateral walls. Most tumors present as a single, large polypoid mass, ranging in diameter from 1.5 cm to 12 cm.1 Grossly, these tumors tend to be polypoid and ulcerated, and most patients with carcinosarcoma of the urinary bladder have an advanced stage of the disease, with muscularis mucosa involvement typically present at the time of initial diagnosis.1 As a result, the diagnosis of sarcomatoid carcinoma using light microscopy alone can be difficult, especially with the small fragments of biopsied specimens or undifferentiated spindle cell tumors without obvious glandular differentiation. In other words, it is difficult to distinguish sarcomatoid carcinoma from sarcomas that have more frequent spindle cell areas, such as carcinosarcoma, leiomyosarcoma, malignant fibrous histiocytoma, and malignant melanoma. To establish a more effective sarcomatoid carcinoma diagnosis, the sarcomatous component should show obvious epithelial differentiation with no heterogeneous mesenchymal components. Carcinosarcoma of the urinary bladder is an aggressive neoplasm that has a mortality rate of approximately 50%. Lopez-Beltran et al. reported that in 26 cases of sarcomatoid carcinoma originating in the bladder, 81% of the patients died within 9.8 months.7 Most patients died either from a local disease or of lymph node, lung, pleura, brain, liver, or bone metastases. Because of the aggressive nature of this neoplasm and its tendency for local recurrence, radical cystectomy seems to be the treatment of choice for patients with sarcomatoid carcinoma of the urinary bladder, although patients often tend to experience local recurrence after surgery.3,10 Alternative treatments such as adjuvant radiotherapy and various combinations of chemotherapy (cisplatin and gemcitabine) have yielded inconsistent results. Therefore, no specific guidelines regarding adjuvant therapy have been described. In the present case, the patient had a severe gross hematuria just 1 month after his operation, and died 1 month later. On the basis of this experience, we confirm that sarcomatoid carcinoma indeed has an early metastasis with a high invasion of neighboring tissues. As a result, if a rapidly growing tumor is detected that seems to originate from the kidney and extends to the ureter and bladder, even though it is rare, sarcomatoid carcinoma should be included in the differential diagnosis. The experience in this case emphasizes that sarcomatoid carcinoma in the urinary bladder should be managed as a highly aggressive tumor with poor outcome requiring more aggressive therapy.


 XML Download
XML Download