

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Renal cell carcinomas (RCCs) can metastasize to almost any organ. The most common involved sites, in order of frequency, are the lung, lymph nodes, liver, contralateral kidney, and bone. RCC involvement of the ipsilateral adrenal gland is noted in 1.2~10% of radical nephrectomy specimens,1 but the sole involvement of the contralateral adrenal gland as the site of metachronous metastasis is rare.2 Here we present an exceptional case of metachronous solitary adrenal metastasis that was treated by retroperitoneal laparoscopic adrenalectomy.
Case Report
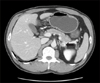
A 40-year-old man presented to our hospital with an incidentally detected right renal mass. Abdominal and pelvic computed tomography (CT) showed a 5×4.7 cm sized mass with mixed attenuation arising from the superior aspect of the right kidney. No other intraabdominal or adjacent organ involvements were found on CT. The patient underwent retroperitoneal laparoscopic radical nephrectomy and ipsilateral adrenalectomy. The pathology report showed RCC (clear cell type) with a Fuhrman nuclear grade of 2. The tumor had not extended into the perinephric fat, adrenal gland, or left renal vein (stage T1bN0M0). Thus, the patient was followed with annual chest X-rays and abdominal CT. Four years after a right nephrectomy, follow-up abdominal CT revealed a 1.3 cm sized enhanced mass in the left adrenal gland (Fig. 1). In addition, positron emission tomography revealed a fluorodeoxyglucose (FDG)-avid, enlarged left adrenal gland with no other abnormality. Endocrinological evaluation demonstrated normal urinary 17-ketosteroids, 17-hydrocorticoids, metanephrines, cortisol, and vanillylmandelic acid.
The patient underwent retroperitoneal laparoscopic left adrenalectomy. The operative time was 2 hours 3 minutes and estimated intraoperative blood loss was 70 ml. Postoperatively, immediate steroid replacement therapy with prednisolone 2.5 mg and fludrocortisones 0.1 mg was given in the morning for adrenal insufficiency. The histological features of the specimen were consistent with the primary RCC, which had not invade d the adjacent structure (Fig. 2).
The postoperative period was uneventful, and the patient was discharged on postoperative day 3. After 1 month, the patient is being treated with interferon monotherapy.
Discussion
Approximately 25% of patients with RCC will already have multiple distant metastases at the time of presentation, including the lungs, lymph nodes, liver, bones, contralateral kidney, and less frequently, the adrenal glands.3 The prevalence of RCC involvement of the ipsilateral adrenal gland is 19% in autopsy series and 5.5% in surgical series, whereas the contralateral adrenal is involved in up to 11% of autopsy series and 3.4% of surgical series with a variability of latency in diagnosis.4,5
Although primary RCC metastasis to the adrenal glands is generally hematogenous because of the rich blood supply of the adrenal gland and its high ratio of blood volume to unit weight,6 and the risk of ipsilateral adrenal metastasis is associated with advanced stage tumors of the upper pole, the predisposing factor for contralateral adrenal metastasis by RCC is still unknown.4 Of particular interest, Stein et al.7 reported that metastatic spread to the contralateral adrenal gland showed an 80% incidence of involvement of the renal vein or inferior vena cava by primary RCC. In our case, preoperative imaging of the RCC before retroperitoneal laparoscopic radical nephrectomy revealed stage I disease.
The most favorable diagnostic approach to a solitary contralateral adrenal tumor in patients with a history of RCC is contentious.4 Radiological studies may facilitate the preoperative diagnosis but cannot determine with certainty whether an adrenal tumor in a patient with RCC is a primary adrenal neoplasm, an adrenal cortical adenoma, or a metastasis.4 The preoperative diagnosis of contralateral adrenal metastasis begins with high suspicion based on a history of RCC. In these patients, the findings of a solitary adrenal tumor without elevated serum adrenal hormones is strongly suggestive of a metastatic lesion to the adrenal gland,7 as in our patient.
Oncologically, surgical removal of a solitary adrenal metastasis remains the only treatment option for these patients. Only surgical treatment can achieve satisfactory survival rates. However, it is difficult to estimate overall survival because of the small number of such cases. Some authors have reported that adrenal metastasectomy can achieve a good rate of freedom from disease after surgery and acceptable survival rates when compared with diffuse metastatic disease.2 Kessler et al8 reported that the longer the interval between nephrectomy and the appearance of the adrenal metastasis, the better the prognosis. Probably this latency in the appearance of metastasis represents a less aggressive behavior of cancerous cells, with slower progression that connotes a better prognosis. These results could justify the indication for surgical resection of adrenal metastasis from RCC with subsequent adjuvant therapy with biological response modifiers.
Recently, laparoscopic adrenalectomy has been performed successfully transperitoneally and retroperitoneally to treat a variety of adrenal pathological conditions. Compared with the transperitoneal approach,9 the retroperitoneal approach is technically simple, can be performed quickly, and has low postoperative morbidity and should be regarded as the routine approach for relatively small adrenal tumors that are less than 5 cm in diameter.10 It also avoids invading the intraperitoneal cavity and possible injury to the abdominal organs. In our case, a patient with a previous history of retroperitoneal laparoscopic radical nephrectomy of the contralateral kidney, the adrenal metastasis measured 1.3 cm in CT and was resected successfully through a laparoscopic retroperitoneal approach.
In conclusion, solitary metachronous contralateral adrenal metastases from RCC are rare clinically, but patients may benefit from the surgical resection of contralateral adrenal metastasis from renal carcinoma. In this case, retroperitoneal laparoscopic adrenalectomy is feasible.

 XML Download
XML Download