

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Acute myocardial infarction without angiographic evidence of arteriosclerosis is uncommon. We report the case of a 63-year-old female patient with acute myocardial infarction. Coronary angiography showed thrombotic total occlusion in the mid left anterior descending artery and thrombotic critical stenosis in the proximal left circumflex artery. Despite multiple balloon angioplasty and aspiration of thrombi, distal flow in the left anterior descending and left circumflex arteries only improved slightly, because abundant thrombi remained. No residual stenosis was observed on angiography. However, computed tomography of the abdomen showed a 5-cm low-attenuated mass with a peripheral enhanced rim in the pancreas and a maximal 7-cm multiple ill-defined peripheral enhanced low-attenuated mass in the liver. Unfortunately, the patient experienced multiple embolic cerebral infarctions 7 days later. The patient had no relevant cardiovascular disease risk factors, signs of heart failure, or arrhythmia. We believe that the pathogenetic mechanism responsible for myocardial infarction in this patient was in situ thrombosis.
Figures and Tables
 | Fig. 1Electrocardiography showed extensive ST elevation in V2 to V6 and I, aVL and marked T inversion in III, aVF compatible with acute anterolateral myocardial infarction.
|
 | Fig. 2Coronary angiogram (CAG) via right transradial approach showed thrombotic total occlusion in midddle left anterior descending artery (LAD) with poor collateral circulation (A) and large thrombotic burden in proximal left circumflex artery (LCX) birfucation site (B). After successful wiring, POBA (plain old balloon angioplasty) was performed using 2.0 mm and 3.0mm sized balloon catheter for LAD and LCX several times. And, aspiration of thrombi using Thrombuster suction device was performed many times (C). Final CAG showed markedly improved flow of LAD and LCX, but distal embolic occlusions in LAD, LCX, and OM (Obtuse marginal) branch were observed (D,E). Small amount thrombi were aspirated by suction catheter (F).
|
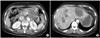 | Fig. 3Computed Tomography (CT) scan of abdomen showed enlarged body and tail of pancreas with 5×5cm sized heterogenous soft tissue mass with multiple lymph node enlargement (A) and multiple metastatic mass (maximum 7 cm sized) in liver (B).
|
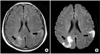 | Fig. 4Axial T2WI (T2-weighted imaging) MR (Magetic Resonance) image (Fast spin echo;FLAIR=Fast fluid-attenuated inversion-recovery) showed Increased signal intensity in left parietal and right occipital lobe (A), and Axial DWI (Diffusion-weighted) MR showed diffusion restriction in the same areas (B).
|
References
1. Rickles FR, Falanga A. Molecular Basis for the Relationship Between thrombosis and Cancer. Thromb Res. 2001. 102:215–224.

2. Brenner B. Arterial thrombotic syndromes in cancer patients. Haemostasis. 2001. 31:Suppl 1. 43–44.
3. Brazdzinomyte J, Mickevicine A, Gailys R, Unikas R, Andriulis M, Macas A. Presentation of rare clinical case of myocardical infarction, induced by neoplasmal obturation of coronary artery. Medicana. 2002. 38:631–636.
4. Braun S, Schrotter H, Reynen K, Schwencke C, Strasser RH. Myocardial infarction as complication of lt atrial myxoma. Int J Cardiol. 2002. 101:115–121.
5. Selvanayagam JB, Iler MA, McRitchie RJ. Coronary thrombosis due to malignancy-induced thrombophilia. Inter Med J. 2002. 32:268–270.
6. Robinson BW, Lewis RR. Myocardial metastasis from carcinoma of pancreas presenting as acute myocardial infarction. J R Soc Med. 1982. 75:560–562.
7. Chen L, Li Y, Gebre W, Lin JH. Myocardial and cerebral infartion due to nobacterial thrombotic endocarditis as an initial presentation of pancreatic adenocarcinoma. Arch Pathol Lab Med. 2004. 128:1307–1308.
8. Gross CM, Posch MG, Geier C, Olthoff H, Krämer J, Dechend R, et al. Subacute coronary stent thrombosis in cancer patient. J Am Coll Cardiol. 2008. 51:1232–1233.
 XML Download
XML Download