

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Many studies have shown that extracorporeal cardiopulmonary resuscitation (ECPR) has favorable outcomes for treating cardiac arrest, particularly in-hospital cardiac arrest (IHCA).1)2)3)4)5)6)7) The overall rate of survival at discharge is 32–45%,1)2)3)4)5)6)7) and a favorable neurologic outcome (cerebral performance category [CPC] of 1 or 2) rate of 77–100% has been reported among survivors.2)3)4)5)6)7) Although these studies might have publication bias, and there is currently insufficient evidence to recommend routine ECPR for cardiac arrest, ECPR could potentially reverse cardiac arrest if it is rapidly implemented.8) Some reports have shown that rapid implementation of ECPR was related to favorable outcomes.9)10)11)
However, a dedicated ECPR team is essential for rapid implementation of ECPR. Ideally, the team should be available full-time in the hospital and respond immediately to ECPR calls. At our institution, there are unfortunately only 2 extracorporeal membrane oxygenation (ECMO) specialists and 2 perfusionists; therefore, they cannot respond immediately to all ECPR calls. In this circumstance, the duration of conventional cardiopulmonary resuscitation (CPR) is usually prolonged, without return of spontaneous circulation (ROSC). This scenario might be similar in other hospitals worldwide. Therefore, we reviewed the effects of ECPR for prolonged, refractory IHCA in order to evaluate the survival rate and neurologic outcome of these patients.
METHODS
Patients
A total of 82 patients underwent ECMO (CAPIOX EBS®; Terumo, Tokyo, Japan) at our institution between July 2011 and December 2015. Of these, 23 patients underwent ECPR for IHCA. Among these, we excluded 4 patients who received ECPR immediately after cardiac arrest, from an ECMO team that was already activated before the arrest occurred. We excluded another 3 patients who did not undergo subsequent therapeutic hypothermia. Finally, we identified 16 patients who met the enrollment criteria (Figure 1). The primary outcome of the study was in-hospital mortality, and the secondary outcome was 1-year survival.
 | Figure 1Enrollment criteria (July 2011 to December 2015).
ECMO = extracorporeal membrane oxygenation; ECPR = extracorporeal cardiopulmonary resuscitation.
|
This study was approved by our Ethics Committee/Institutional Review Board, which waived the requirement for informed patient consent because of the retrospective nature of the analysis.
Treatment protocol
ECPR is indicated in suspected cardiac arrest if the following criteria are met: 1) age <75 years, 2) no-flow time <5 minutes, and 3) ROSC for less than 30 minutes without uncontrollable bleeding, previous severe neurologic deficit, previous end-stage organ failure, or current intracranial hemorrhage. These criteria are in alignment with current recommendations12)13)14) but are not an absolute indication.
Our ECPR team consists of one cardiac surgeon, one assistant (resident, intern, or nurse), and one perfusionist. They are not stationed in the hospital but are required to live within 30 minutes of the hospital. During CPR, an attending physician calls the cardiac surgeon to discuss whether ECPR should be performed, and the surgeon activates the team. While the team arrives, the physician obtains informed consent for ECPR from the patient's family, if available.
We routinely insert cannulas in the right femoral artery and vein using the percutaneous technique, with or without ultrasound guidance. We open the left inguinal area and expose the femoral vessels to insert the cannulas in cases of failed cannulation. After guide wire insertion, 3,000 units of unfractionated heparin are infused intravenously; cannulation is performed using an 18-Fr arterial cannula (OptiSite®; Edward Lifesciences, Irvine, CA, USA) and a 20-Fr venous cannula (VFEM®; Edward Lifesciences). The circuit is primed with normal saline and 1,000 units of unfractionated heparin during cannulation. A chest radiograph is used to monitor and adjust the venous cannula tip position at the level of the carina. Transthoracic echocardiography is performed when sufficient circulatory support is established, followed by a coronary angiography or a computed tomography scan, depending on the suspected cause of arrest.
ECMO target parameters include cases when: 1) the bypass flow is as high as possible if the drainage is adequate and the cardiac index is usually between 2.0 and 2.8 L/min/m2, 2) mean arterial pressure between 50 and 70 mmHg, 3) arterial pulse pressure >10 mmHg without left ventricular distension or pulmonary edema, and 4) decrease and normalization of serum lactate level. Activated clotting time is maintained between 160 to 200 seconds by adjusting the intravenous heparin infusion dose. However, in patients with active bleeding, heparin is discontinued until the bleeding is stopped. If the cannulated limb is pale, we insert a 5-Fr catheter at the cannulated superficial femoral artery for distal perfusion. In the case of pulmonary edema without pulse pressure, because of severe left ventricular dysfunction, an intravenous epinephrine infusion is added to facilitate ventricular contraction. Invasive procedures such as interatrial septostomy or left ventricular venting cannula insertion are not routinely performed to decompress the left ventricle for patients with contraindications.
Therapeutic hypothermia is routinely performed in unresponsive patients (Glasgow Coma Score ≤8) with IHCA treated with ECPR. The ECMO machine at our hospital (CAPIOX EBS®; Terumo) is not equipped with a cooling device, so patients are cooled with an endovascular cooling catheter (Alsius®; Zoll Medical Corp., Chelmsford, MA, USA) placed in the inferior vena cava via a femoral venous sheath or cooled with a surface cooling pad device (Arctic Sun®; Bard Medical, Louisville, CO, USA) applied to the patient's chest and limbs. The cooling procedure is initiated as soon as the catheter or cooling pad is installed and continued until the core body temperature reaches 34.5–35.0°C. The target temperature is 34.5°C to avoid overcooling and complications. Shivering during mild therapeutic hypothermia is evaluated using the Bedside Shivering Assessment Scale, and patients with a score >1 are treated with deeper sedation or with a bolus of intravenous meperidine and muscle relaxant in refractory cases.15) The core body temperature is recorded every hour with a thermometer at the tip of an esophageal probe. Hypothermia is maintained for 48 hours, and gradual rewarming is initiated. The target rate of rewarming is 0.5°C of temperature elevation every 12 hours.
ECMO flow is reduced gradually to 1 L/min and maintained for at least 12 hours when improved cardiac function is confirmed using a transthoracic echocardiography. Heparin treatment is discontinued, and the cannulas are removed after 4 to 6 hours if the patient is hemodynamically stable and the lactate level is not increasing. The cannulas are removed, and the sites are manually compressed for 1 hour if they are inserted percutaneously; however, if the cannulas are inserted through skin incision, they are removed, and the femoral vessels are repaired surgically using 5-0 monofilament non-absorbable sutures.
Statistical analysis
Categorical variables are presented as numbers and percentages and were compared using the χ2 and Fisher's exact tests. Continuous variables are expressed as the mean±standard deviation (SD) and were compared using Student's t-test or the Mann-Whitney U test. The survival rate was estimated with the Kaplan-Meier method. All reported p values were 2-sided, and p<0.05 was considered statistically significant. SPSS version 19 (SPSS Inc., Chicago, IL, USA) was used for statistical analyses.
RESULTS
Baseline patient characteristics
The baseline characteristics of the study population are shown in Table 1. One patient underwent off-pump coronary artery bypass (OPCAB) grafting 2 days prior to the procedure, for myocardial infarction. All patients received by-stander CPR, and the “no-flow” time (time between arrest and CPR start) was too short to measure. The mean “low-flow” time (time between CPR start and bypass start) was 66.5±29.9 minutes, and the minimum value was 39 minutes. The emergency unit (n=6) and the angiography room (n=6) were the most frequent ECPR sites. Out of the 2 patients who received ECPR in the intensive care unit (ICU), one underwent a percutaneous coronary intervention (PCI) just before the arrest, and the other underwent OPCAB grafting 2 days before ECPR. One patient received ECPR in the operating room (OR) during the ventilator weaning period after a rotator-cuff surgery. He had received coronary stenting at the left anterior descending (LAD) branch 5 years prior to undergoing ECPR. In the general ward, one patient received CPR 18 days after a flap surgery for diabetic foot. This patient underwent balloon angioplasties on the left circumflex and right coronary arteries under CPR, followed by ECPR. The baseline characteristics were not different between survivors and non-survivors.
Table 1
Baseline characteristics

COPD = chronic obstructive pulmonary disease; CPR = cardiopulmonary resuscitation; ICMP = ischemic cardiomyopathy; ICU = intensive care unit; OR = operating room; ROSC = return of spontaneous circulation; VF = ventricular fibrillation; VT = ventricular tachycardia.
*Time between CPR start and bypass start.
![]()
Early outcomes and follow-up
Early outcomes are summarized in Table 2, and all patient clinical data are presented in Table 3. Myocardial infarction was the most common cause of arrest (87.5%). Mortality primarily occurred within the third day (75%) of ECPR. A total of 8 patients died before discharge (mortality group); among them, 7 patients died on ECMO. Of these 7 patients, 3 died on the day of ECPR, and another 3 died 2 or 3 days after the procedure. In the mortality group, a patient (patient 16, Table 3) died from uncontrollable bleeding from the sternotomy site that was made for central cannulation. The Methods section describes the frequency of procedures; invasive procedures such as central ECMO to decompress the left ventricle are not routinely performed in patients with contraindications. This patient, however, was alert and young (55-year-old) but showed pulmonary edema and limb ischemia on peripheral ECMO. Based on this, peripheral ECMO was replaced with central ECMO. Another 58-year-old female patient (patient 12, Table 3) with ischemic cardiomyopathy (ICMP) was rescued with ECPR and was weaned off ECMO 51 hours after. Twenty days later, however, she died from heart failure, and her family did not want further CPR to be performed.
Table 2
Early ECPR IHCA outcomes
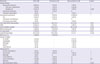
CPC = cerebral performance category; CRRT = continuous renal replacement therapy; ECMO = extracorporeal membrane oxygenation; ECPR = extracorporeal cardiopulmonary resuscitation; ICU = intensive care unit; IHCA = in-hospital cardiac arrest; LVEF = left ventricular ejection fraction; PCI = percutaneous coronary intervention; ROSB = return of spontaneous beating; VD = vessel disease.
*Death on ECMO; †death after ECMO weaning.
![]()
Table 3
Clinical data of all patients

AMI = acute myocardial infarction; Angio = angiography room; CPRT = continuous renal replacement therapy; ECMO = extracorporeal membrane oxygenation; ECPR = extracorporeal cardiopulmonary resuscitation; ER = emergency room; ICMP = ischemic cardiomyopathy; ICU = intensive care unit; LAD = left anterior descending; LM = left main disease; OPCAB = off-pump coronary artery bypass; OR = operating room; PCI = percutaneous coronary intervention; Pt. = patient; PTE = pulmonary thromboembolism; VD = vessel disease; VF = ventricular fibrillation; VT = ventricular tachycardia.
*Worst value before ECPR.
![]()
Eight patients survived to discharge (survival group) with favorable neurologic outcomes (CPC 1–2). Of these, 7 patients had CPC 1. In the survival group, a patient (patient 1, Table 3) underwent fasciotomy followed by Achilles tendon lengthening because of limb ischemia, and another patient (patient 7, Table 3) underwent Achilles tendon lengthening alone because of ankle contracture. Two patients (patient 1 and 5, Table 3) experienced newly onset heart failure. Patient 5 died one year after discharge, and patient 1 is still alive 5 years after ECPR and waiting for heart transplantation.

DISCUSSION
We identified the impact of ECPR followed by therapeutic hypothermia on survival and neurologic outcome in patients with prolonged, refractory IHCA. Rates of survival and poor neurologic outcome of conventional CPR for patients with IHCA are currently low. Survival to discharge was 15%, and only 50% of these survivors had favorable neurologic outcomes (CPC scale 1 or 2).16) However, ECPR was associated with increased survival benefits compared with conventional CPR in patients with IHCA who received refractory to conventional CPR for more than 10 minutes.5)
Risk factors associated with in-hospital mortality in ECPR have been reported in previous studies, including initial rhythm as pulseless electrical activity or asystole, long “low-flow” time, low serum pH, and high serum lactate.1)3)4) In practice, however, these factors, with the exception of reducing the “low-flow” time, cannot be controlled by the ECMO team. Some reports have indicated that rapid implementation of ECPR can improve cardiac arrest outcomes and can be considered for potentially reversible cardiac arrest if rapidly implemented.8)9)10)11) Kim et al.17) reported that every 10-minute increment in low-flow time increased the rate of mortality by 5%, and an amount of time less than 60 minutes is important for improving survival outcomes. Based on these results, they recommended that the team and machine be prepared to respond rapidly to these events. In the real world, although it is necessary to have many specialists in the hospital for rapid ECPR implementation, most institutions cannot afford this staffing model. In these circumstances, the duration of “low-flow” time tends to be prolonged (66.5±29.9 minutes with a minimum of 39 minutes in our study), even if arrest occurs in the hospital, and it is very difficult to determine if ECPR should be performed.
A few studies have evaluated the use of therapeutic hypothermia in adult patients that receive ECPR.2)9)14)18) Based on these studies, therapeutic hypothermia as a bundle therapy is being established as a recommended procedure.19) However, the ideal target temperature, initiation, and duration of therapeutic hypothermia for treating patients who received ECPR for IHCA have not been well-established. We selected a target temperature of 34.5°C to avoid unexpected bleeding complications, while still maintaining the neuroprotective effect of mild therapeutic hypothermia.20)
In this study, we worked to reflect realistic clinical scenarios from team activation to the start of bypass and excluded 4 patients who received ECPR immediately after cardiac arrest from an ECMO team that was already activated before the arrest occurred. As mentioned previously, we have 2 ECPR teams, and each consists of one cardiac surgeon, one assistant (resident, intern, or nurse), and one perfusionist. The teams are not stationed in the hospital but live within 30 minutes travel time from the hospital. Under these circumstances, the “low-flow” time in our study was relatively long (66.5±29.9 minutes with a minimum of 39 minutes), but the rate of survival to discharge with a favorable neurologic outcome (50%) was comparable with other reports.1)2)3)4)5)9)10)11) In our experience, it usually takes about 20 minutes to prepare the machine and perform cannulation, but we were unable to measure the exact time because of insufficient medical records.
The most common cause of mortality was failure to achieve return of spontaneous beating after the bypass was started (37.5%). All of these patients (n=3) died within the first 27 hours after the procedure because heart transplantation or a ventricular assist device was not available, and there were no other options except termination of ECMO. The mean “low-flow” time in patients who died from failure to achieve return of spontaneous beating was 53.7±14.2 minutes, and this result was not significant compared with the mean “low-flow” time for the other patients (69.5±32.1 minutes). The severity and extent of myocardial damage are more important risk factors for failing to achieve return of spontaneous beating than the duration of “low-flow” time. However, we were unable analyze this result because of the small population and retrospective design of this study.
As mentioned above, some risk factors associated with in-hospital mortality have been reported in previous studies, including initial rhythm as pulseless electrical activity or asystole, long “low-flow” time, low serum pH, and high serum lactate.1)3)4) In our study, however, the severity of lactic acidosis and duration of “low-flow” time were not identified as risk factors for in-hospital mortality. This might be attributable to the small study population and retrospective design of this study.
This study is limited by the retrospective analyses of observational data and only included 16 patients and no control group, so a comparative study could not be performed. Therefore, these results did not completely show the effectiveness of therapeutic hypothermia or ECPR. The decision to implement ECPR was affected by the attending physician's preference, producing selection bias. Further prospective studies with larger cohorts are needed to confirm our results.
In conclusion, ECPR in combination with therapeutic hypothermia could be considered in prolonged refractory IHCA if bystander-initiated conventional CPR is performed, even if the team does not reside in the hospital.
 XML Download
XML Download