

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Heart failure (HF) is a common health problem associated with frequent hospitalization, reduced quality of life and high post-discharge mortality.1) Despite advances in drug and device therapies for chronic heart failure with reduced ejection fraction (HFrEF), outcomes remain suboptimal. Functional impairment is one of the major determinants of quality of life in patients with HFrEF. Functional capacity varies significantly among HFrEF patients, and it remains unclear why functional capacity is compromised in some patients with HFrEF while it is preserved in others. Left ventricular ejection fraction (LVEF) correlates strongly with mortality in these patients.2) However, in daily clinical practice, LVEF does not always reflect functional capacity in patients with HFrEF.3)4)5) Besides reduced LVEF, specific pathological mechanisms such as secondary pulmonary hypertension, right ventricular (RV) dysfunction, left ventricular (LV) diastolic dysfunction, and subsequent valvular diseases are common in HFrEF and might affect prognosis.2)6) Due to chronic elevation of the LV filling pressure, the pulmonary vasculature may undergo some reactive changes such as intimal fibrosis, medial hypertrophy, and abnormalities of the elastic fibers, resulting in remodeling of the arterial wall and reactive increases in pulmonary vascular resistance.7)
Pulmonary artery stiffness (PAS) has been developed as a relatively new Doppler echocardiographic parameter to evaluate the pulmonary arterial vasculature and mechanics.8) Although its association with RV function and ability to predict functional capacity in pulmonary hypertension has been demonstrated, data regarding its association with functional status in patients with HFrEF without pulmonary hypertension or right HF has not been fully evaluated.9)10)11) In this study we sought to evaluate the association between PAS and functional capacity in patients with HFrEF.
METHODS
Study population
This cross-sectional observational study was conducted in the outpatient clinic of the cardiology department of our institution. A total of 46 patients with HF and 52 controls were enrolled in the study. HF patients with LVEF ≤45% on echocardiography, and who were clinically stable for at least one month before enrollment were included in the study. Due to the previously defined relationship between PAS and pulmonary hypertension or right HF,9)10)11) patients with right HF or dilatation and pulmonary hypertension (tricuspid jet velocity >2.8 m/sec) were excluded from the study. The criteria for right HF or dilation used to exclude patients were RV dimensions >41 mm at the base, >35 mm at the midlevel on the RV-focused view and tricuspid annular plane systolic excursion (TAPSE) <17 mm.12) Moderate-to-severe valvular heart disease, newly-diagnosed HF (<6 months), ventricular arrhythmias, constrictive pericarditis, sleep apnea syndrome, acute and chronic lung disease, connective tissue disease, congenital heart disease, chronic thromboembolic pulmonary hypertension, thyroid dysfunction, and anemia (with hematocrit lower than 35%) were also excluded. In addition, 52 individuals who were New York Heart Association (NYHA) class I and age-sex matched to the HFrEF group served as controls. Subjects were informed regarding the purpose of the study and written informed consent was obtained. The local ethics committee of our institution approved the study protocol.
Detailed family and medical history were obtained from all patients meeting the inclusion criteria. NYHA functional capacity and medical therapies were recorded. Physical examination, 12-lead electrocardiography (ECG) and laboratory investigations including complete blood count, blood biochemistry, and thyroid function tests were routinely performed for all patients.
Echocardiography and PAS
Transthoracic echocardiography was performed using a Philips iE33 6.0 ultrasound system (Philips Medical Systems, Andover, MA, USA) with a 2.5-MHz phased-array transducer in the left lateral decubitus position at the end of expiration. All echocardiographic assessments were performed based on recommendations of the American Society of Echocardiography guidelines.12) LVEF was calculated using the modified Simpson's rule. All data were stored digitally and reanalyzed off-line by 2 physicians who were blinded to group enrollment.
PAS was assessed in the parasternal short-axis view using pulsed-wave Doppler recording of pulmonary flow at one centimeter distal to the pulmonic valve annulus at a speed of 100 mm/sec. Subsequently, the Doppler frequency shift, acceleration time (AcT), maximum flow velocity (MFV), and velocity time integral of Doppler flow trace of the pulmonary artery were measured. To prevent the potential effects of breathing and cardiac cycle on measurements, the average of at least 3 consecutive Doppler flow traces was evaluated for each parameter. PAS was calculated the ratio of MFV shift of pulmonary flow (MFV) to pulmonary acceleration time (AcT) according to the following formula (Figure 1)8):

Statistical analysis
All statistical analyses and calculations were conducted using the SPSS 20.0 Statistical Package Program for Windows (SPSS Inc., Chicago, IL, USA). Continuous variables are expressed as mean±standard deviation (SD) and categorical variables as percentages. To test the normalization of data distribution Kolmogorov-Smirnov test was used. The χ2 test was used to compare categorical variables. Student's t-test and Mann-Whitney U test were used for continuous variables with and without a normal distribution, respectively. Pearson's and Spearman coefficients were used to analyze correlation of variables with and without a normal distribution, respectively. To determine the independent variables likely to affect the PAS, multivariate linear regression analysis was performed with a backward selection process including parameters that were significant in univariate correlation analysis and variables which were significantly different between two groups. A p value less than 0.050 was considered statistically significant.
RESULTS
Demographic and clinical results
A total of 98 participants, consisting of a patient group of 46 subjects with HFrEF (32 men, 69.6%) and a control group of 52 volunteers (25 men, 48.1%) were included in this study. Demographic, clinical, and laboratory findings of both groups are shown in Tables 1 and 2. The functional class of all HFrEF patients was evaluated. Five patients (10.9%) were in class I, 18 patients (39.1%) were in class II, 18 patients (39.1%) were in class III, and 5 patients (10.9%) were in class IV. The etiology of HFrEF was ischemic heart disease in 31 (67.4%) patients and non-ischemic dilated cardiomyopathy in 15 (32.6%) patients.
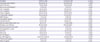
Table 1
Baseline demographic and clinical findings

Data are shown as mean±standard deviation or number (%).
ACEI = angiotensin converting enzyme inhibitor; AF = atrial fibrillation; ARB = angiotensin receptor blocker; BMI = body mass index; CABG = coronary artery bypass graft; CCB = calcium channel blockers; DBP = diastolic blood pressure; HF = heart failure; HFrEF = heart failure with reduced ejection fraction; ICD = implantable cardioverter defibrillator; NA = not applicable; NYHA = New York Heart Association; SBP = systolic blood pressure.
*Data without a normal distribution were compared using the Mann-Whitney U test.
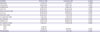
Table 2
Laboratory findings
Data are shown as mean±standard deviation.
eGFR = estimated glomerular filtration rate; ESR = erythrocyte sedimentation rate; HDL-C = high-density lipoprotein cholesterol; HFrEF = heart failure with reduced ejection fraction; hs-CRP = high-sensitive C-reactive protein; LDL-C = low-density lipoprotein cholesterol; MPV = mean platelet volume; Total-C = total cholesterol; WBC = white blood cell.
*Data without a normal distribution were compared using the Mann-Whitney U test.
Echocardiographic results
Echocardiographic measurements of both groups are shown in Table 3. PAS was significantly increased in the HFrEF group compared to the control group (10.53±2.40 vs. 7.41±1.32, p<0.001).
Table 3
Echocardiographic findings
Data are shown as mean±standard deviation or number (%).
E/E' = early mitral filling velocity/early diastolic mitral annular velocity; HFrEF = heart failure with reduced ejection fraction; IVC = inferior vena cava; IVSd = interventricular septum diastole; LA = left atrium; LVEF = left ventricular ejection fraction; LVIDd = left ventricular internal dimension diastole; LVPWd = left ventricular posterior wall diastole; PAS = pulmonary artery stiffness; sTa = tricuspid annular systolic velocity; TAPSE = tricuspid annular plane systolic excursion.
*Data without a normal distribution were compared using the Mann-Whitney U test.
The HFrEF group was further divided into 4 subgroups according to NYHA functional class. In sub-group analysis of patients with HFrEF, PAS significantly differed between groups according to functional class (8.53±2.49 for NYHA class I; 10.04±2.25 for NYHNA class II; 11.03±2.37 for NYHA class III; and 12.50±1.07 for NYHA class IV; p=0.033) (Figure 2). HFrEF patients with poor NYHA functional capacity had higher PAS compared those with good functional capacity. The intra-observer and inter-observer correlation coefficients were 0.96 and 0.95 for PAS, indicating good reproducibility and reliability.
Figure 2
PAS values according to NYHA functional class of HFrEF patients.
HFrEF = heart failure with reduced ejection fraction; NYHA = New York Heart Association; PAS = pulmonary artery stiffness; SD = standard deviation.

We further classified HFrEF patients into 2 groups, low PAS (PAS <8.88 kHz/sec) and high PAS (PAS ≥8.89 kHz/sec) according to the mean value of PAS in our cohort (as there is no established cutoff value). Afterwards, echocardiographic parameters were compared between the 2 groups. Only mitral A (68.50±19.94 cm/sec for patients with low PAS and 53.86±14.38 cm/sec for patients with high PAS, p=0.033) and mitral A' (9.7±3.46 cm/sec for patients with low PAS and 6.87±3.17 cm/sec for patients with high PAS, p=0.038) differed significantly between groups.
Clinical, laboratory, and echocardiographic parameters that were significantly associated with PAS in univariate and multivariate correlation analysis are shown in Table 4. Backward multivariate linear regression analysis including variables that were significant in univariate correlation analysis and variables, which were significantly different between two groups, was performed to determine the independent variables likely to affect the PAS. The included variables were: duration of HF, NYHA class, systolic blood pressure (SBP), age, presence of atrial fibrillation (AF), presence of implantable cardioverter defibrillator (ICD), pro-brain natriuretic peptide (pro-BNP), estimated glomerular filtration rate (eGFR), left atrium (LA) diameter, mitral early mitral filling velocity/early diastolic mitral annular velocity (E/E') ratio, inferior vena cava (IVC) diameter, LVEF, left ventricular internal dimension diastole (LVIDd), and TAPSE. In multivariate linear regression analysis, NYHA class, duration of HF, and LA diameter were found to be independently associated with PAS.
Table 4
Clinical, laboratory and echocardiographic parameters associated with PAS in patients with HFrEF

Only significant correlations with PAS are given in the table. Parameters included in multivariate analysis were: duration of HF, NYHA class, SBP, age, presence of AF, presence of ICD, pro-BNP, eGFR, LA diameter, mitral E/E' ratio, IVC diameter, LVEF, LVIDd, and TAPSE.
AF = atrial fibrillation; CI = confidence interval; E/E' = early mitral filling velocity/early diastolic mitral annular velocity; eGFR = estimated glomerular filtration rate; ESR = erythrocyte sedimentation rate; HDL-C = high-density lipoprotein cholesterol; HF = heart failure; HFrEF = heart failure with reduced ejection fraction; ICD = implantable cardioverter defibrillator; IVC = inferior vena cava; LA = left atrium; LVEF = left ventricular ejection fraction; NYHA = New York Heart Association; PAS = pulmonary artery stiffness; pro-BNP = pro-brain natriuretic peptide; SBP = systolic blood pressure; TAPSE = tricuspid annular plane systolic excursion; Total-C = total cholesterol.
*Data without a normal distribution were compared using the Spearman coefficient. The c-statistic for the model was 0.874.
DISCUSSION
Our study demonstrated that PAS was significantly increased in patients with HFrEF without pulmonary hypertension or right HF and severity of NYHA class was independently associated with PAS. PAS should be considered an underlying pathophysiological mechanism of impaired functional status in patients with HFrEF.
PAS is a new echocardiographic index that can be used to noninvasively evaluate the elastic properties of pulmonary arterial vasculature. Pulmonary artery elasticity is calculated by means of a method used in determining aortic stiffness.8) PAS is a Doppler echocardiographic parameter derived from AcT. Duration of RV systolic ejection time obtained from pulmonary artery systolic wave decreases when pulmonary artery distensibility impairs. This is primarily the result of reductions in AcT of pulmonary flow trace. In a stiff pulmonary artery, a decrease in AcT leads to an increase in velocity and maximum frequency shift.9) In addition, increased PAS leads to a higher RV workload and enhances energy transmission to small pulmonary vessels, which results in further vascular damage.13)14) Increased stiffness or impaired distensibility of the pulmonary artery also diminishes systolic cross-sectional area due to impaired systolic expansion.
Increases in PAS were previously reported to result from many clinical conditions affecting the right heart chambers.9)10)15)16)17)18)19)20)21) The relationship between PAS and functional capacity in patients with pulmonary hypertension has also been reported.11)19) Although the association between PAS and right heart function and its ability to predict functional capacity in pulmonary hypertension has been demonstrated, data regarding the association between PAS and functional status in patients with HFrEF without pulmonary hypertension or right HF has not been evaluated previously.
In our study, PAS was significantly increased in the HFrEF group compared with the control group. Since subsequent RV dysfunction and secondary pulmonary hypertension are frequently seen in patients with HFrEF,6)22)23) this result was not surprising. In addition, subgroup analysis of patients according to functional status showed that PAS differed significantly among the 4 NYHA classes. In multivariate linear regression analysis, NYHA class was an independent factor associated with PAS.
Symptoms of HF in patients with HFrEF are multifactorial and related not only to LVEF, but also LV diastolic dysfunction, subsequent valvular diseases, secondary pulmonary hypertension, RV dysfunction, and comorbidities. The low resistance of the pulmonary vasculature can initially compensate for elevated pressure despite vigorous ongoing vascular histological changes promoting stiffness. Increased afterload induces RV adaptive remodeling in order to maintain adequate perfusion through the pulmonary circulation.24) Thus, cardiac output and preserved ejection fraction are maintained and lead to mild clinical symptoms in a state of compensated hemodynamic function.25) Whenever progressive elevation in afterload overcomes an adaptive change, RV is dilated as a result of pressure overload and progressive RV failure is observed.26)27) The conventional techniques developed to quantify vascular and cardiac function in a clinical setting are invasive and require complex analysis. Currently, the assessment of proximal PAS is not a routine part of clinical evaluation.28) Clinicians should keep in mind that the estimation of pulmonary artery pressure by echocardiography is not always error-free and, moreover, impairment in RV function may appear regardless of the presence of pulmonary hypertension or overt right HF. Given our findings, increased PAS should warn clinicians of impending functional status compromise even in the absence of right heart dysfunction or pulmonary hypertension. Alterations in PA elasticity can be detected early in the course of the disease using PAS, even before overt pressure elevation. However, its routine use for diagnostic or prognostic purposes will require further studies.
The small number of patients and the single-center nature of the study are the main limitations of this study. The echocardiographic method has not been widely validated to measure PAS and the reproducibility of this technique was not evaluated. Also, there has not been a consensus about the normal range of PAS measured by this echocardiographic method. Echocardiographic evaluation may be more comprehensive when used simultaneously with right heart catheterization or cardiac magnetic resonance imaging (MRI). Although NYHA functional class is used worldwide in patients with HF, there is notable interobserver variability. In addition, the 6-minute walking test and cardiopulmonary exercise test were not performed for evaluation of functional capacity. Large multicenter studies will be needed to definitively characterize pulmonary artery elasticity in patients with HFrEF.
In conclusion, PAS is associated with functional status and should be taken into consideration as an underlying pathophysiological mechanism of impaired functional status in patients with HFrEF without overt pulmonary hypertension or right HF. However, our findings need to be confirmed by future studies including a large number of patients and a long-term follow-up period before implementing PAS in everyday practice.
 XML Download
XML Download