

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The presence of left ventricular hypertrophy (LVH) can heighten the risk of cardiovascular disease and mortality.1)2)3) LVH is frequently observed in hypertensive patients and has been considered an adaptive response to hemodynamic overload imposed by systemic hypertension.4) Although hypertrophic growth of cardiomyocytes is the chief mechanism for LVH, other pathologic mechanisms concurrently exist, including fibroblast proliferation and exaggerated accumulation of collagen fibers within the interstitium and perivascular regions, which provokes additional development of fibrosis and left ventricular (LV) dysfunction.5) Stiff cardiomyocytes and increased collagen deposition can trigger LV diastolic dysfunction — the major cardiac functional deficit in heart failure with preserved ejection fraction (EF).6)
Prior studies have documented that aortic calcium scoring is an independent prognosticator of cardiovascular events.7)8) Despite a well-known association between vascular calcification and clinical outcome, it remains unclear whether calcification has a direct impact on clinical outcomes or is merely a marker of atherosclerotic burden for each individual. We have previously reported that heavy aortic calcification and resultant arterial stiffening could be underlying causes of LVH and diastolic dysfunction in older-aged male patients that present with hypertension.9) Because myocardial afterload excess is currently thought to be a possible mechanism of diastolic heart failure, along with the progression of LVH,6) patients with LVH are more likely to experience symptoms of heart failure, as well as unfavorable clinical outcomes, in light of an increased afterload associated with a stiffened aorta due to heavy aortic calcification.
This study investigated the predictive utility of aortic calcification, a reflection of aortic stiffness, to determine if stiffness differed based on the presence of LVH. Specifically, we hypothesized that the impact of thoracic aorta calcium score (TACS) on clinical outcomes would be more profound in those with LVH, given that diseased myocardium is more likely to be vulnerable to afterload increase associated with aortic stiffness.
METHODS
Study population
We retrospectively reviewed a sample of 1,578 elderly individuals who were 65 years of age or above and who underwent concurrent coronary computed tomography (CT), exercise treadmill testing, and echocardiography to evaluate suspected coronary artery disease (CAD). The tests were performed within 90 days during 2003 through 2009 at Severance Cardiovascular Hospital, Seoul, Korea. Study individuals were excluded if they presented with obstructive CAD on coronary CT (luminal stenosis ≥50%), if their CT scan did not include the entire thoracic aorta from the aortic arch to diaphragm level, if they did not complete a minimum of 2 stages of the Bruce protocol exercise treadmill test, or if they reported the presence of atrial fibrillation, LVEF <50%, significant valvular dysfunction, or LVH related to either hypertrophic cardiomyopathy or infiltrative disease. Overall, 487 study individuals without obstructive CAD or LV systolic dysfunction were included in the analytic sample. The median number of days between coronary CT scans and exercise treadmill testing or echocardiography was 7 days (interquartile range [IQR], 2–14 days) and 8 days (IQR, 2–18 days), respectively. The appropriate institutional review committee at Severance Hospital, Yonsei University in Seoul, Korea approved this study.
Clinical examination
Clinical data were ascertained at baseline from routine medical history questionnaires, physical examination, and laboratory testing. In brief, body mass index (BMI) was calculated from height and weight measures. Diabetes mellitus was defined as receiving anti-diabetic treatment or a fasting plasma glucose of 126 mg/dL or more. Current cigarette smoking was defined as any cigarette smoking in the past month. Hypertension was defined as systolic blood pressure (SBP) ≥140 mmHg and/or diastolic blood pressure (DBP) ≥90 mmHg or use of antihypertensive agents. Dyslipidemia was defined as the use of cholesterol-lowering medication or a serum total cholesterol level of 200 mg/dL or more.
CT protocol and image acquisition
Patients were scanned using a 64-section CT scanner (Sensation 64; Siemens Healthineers, Forchheim, Germany). For calcium scanning, unenhanced CT was performed with prospective electrocardiography-triggered acquisitions in mid-diastole using 120–140 kV with 150–220 mAs, depending on the patient's size; 240 milliseconds exposure time per rotation; 330 milliseconds gantry rotation time; and 64×0.6 mm slice collimation. Calcium scans were reconstructed at 70% of the R-R interval using a slice thickness of 3 mm with an increment of 3 mm. Coronary artery calcium score (CACS) and TACS were measured on reconstructed images. Foci of the coronary artery, aortic valve, and thoracic aorta were identified and scored by an experienced technician who was blinded to the patient's medical records, using semi-automatic software (Vitrea 2.0; Vital Images, Minnetonka, MN, USA). Lesion-specific calcium scores were summed across all lesions identified within the left main, left anterior descending, left circumflex, and right coronary arteries to provide the CACS. In addition, the TACS included calcium that was scored in the ascending aorta, aortic arch, and descending aorta to the diaphragm level. An objective volume scoring approach included in the system software was determined, which provided a score in cubic millimeters (Figure 1).

Subsequently, coronary CT angiography was performed. Patients without a contraindication to beta-adrenergic blocking agents and with initial heart rate higher than 65 beats/min received a single oral dose of 40 mg propranolol hydrochloride 1 hour before coronary CT angiography. Two types of CT system configurations were employed: 1) a 64-slice CT scanner (Sensation 64; Siemens Healthineers) using retrospective electrocardiogram (ECG) gating with tube current modulation from 2003 through 2009 with the following parameters: rotation time, 330 ms; tube voltage, 100–120 KeV; tube current, 400–800 mA; and pitch factor, 0.2; and 2) a 64-row CT scanner (LightSpeed VCT XT; GE Healthcare, Milwaukee, WI, USA) using a prospectively ECG-gated axial technique from 2008 through 2009 with the following parameters: rotation time, 350 ms; tube voltage, 100–120 KeV; and tube current, 300–900 mA. A real-time bolus-tracking technique was applied to trigger the scan initiation. Radiation doses for the calcium scan and total CT scan were 1.5±0.3 mSv and 10.7±2.8 mSv, respectively.
The intraobserver variability level in the TACS measurement was determined. Measurements were performed by one observer, based on analysis of 100 random images. The observer also performed repeated analysis in an interval of at least one month, while remaining blind to results from the first analysis.
Exercise testing
A symptom-limited exercise treadmill test was performed according to the Bruce protocol.10) Resting SBP and DBP were measured in the brachial artery in the seated position. During the exercise stress test, heart rhythm, SBP, and DBP were recorded at the end of each stage of exercise, at peak stress, and during recovery. ΔSBP was defined as the difference between SBP at rest and peak exercise. Pulse pressure (PP) was defined as the difference between SBP and DBP. ΔPP was defined as the difference in PP between rest and peak exercise. A 12-lead ECG was obtained every minute, and a 3-lead ECG for heart rhythm was monitored continuously. Indications for terminating the exercise treadmill test have been described previously.11)
Echocardiographic measurement
The dimensions of the left ventricle and EF were measured as recommended by the American Society of Echocardiography guidelines.12) LV mass was calculated using the formula as recommended, and LV mass index was defined as the LV mass indexed for body surface area. LVH was defined as an LV mass index >115 g/m2 for men and >95 g/m2 for women.12) Left atrial (LA) volume was calculated by use of standard criteria according to the American Society of Echocardiography recommendations, and the LA volume index was defined as the LA volume indexed for body surface area. Mitral inflow velocities were obtained by pulse wave Doppler in the apical four-chamber view. The mitral early diastolic velocity (E) was also measured. The peak early diastolic mitral annular velocity (e') was measured from the septal mitral annulus; we then calculated the E/e' ratio, which is a measure of the LV filling pressure.
Study endpoint
Study individuals were followed over a median of 65 months (IQR, 17–89 months) for a primary composite end point of cardiac death, inpatient admissions for heart failure, obstructive CAD requiring revascularization or bypass surgery, and stroke. Clinical event occurrence was ascertained by review of hospital records and by telephone interview, if necessary.
Statistical methods
The distributions of relevant variables are reported as mean±standard deviation for continuous parametric variables, median with 25–75% range for non-parametric continuous variables, as necessary, or count with proportion for categorical measures. Both LVH and TACS groups were compared using Student's t-test for continuous variables and the χ2) statistics for categorical parameters. Univariate Cox regression analysis reporting hazard ratio (HR) with 95% confidence interval (CI) was employed to determine independent predictors for the primary composite endpoint. Separate multivariate Cox regression models were generated according to the individually acquired coronary CT measures, as well as subsequent LVH and TACS strata. A Kaplan-Meier survival curve with log-rank test for equality was fashioned to display time-to-events, which were stratified by LVH and TACS groups. The intraclass correlation coefficient (ICC) was calculated to evaluate intraobserver reproducibility. Good correlation was defined as an ICC >0.8. A p value <0.050 was considered statistically significant.
RESULTS
Overall, the median value of TACS was 446 mm3 (IQR, 132–1,223 mm3). Patients were divided into 4 groups according to the presence of LVH and TACS value. Low and high TACS values were defined as lower and higher TACS in comparison to median TACS, respectively. Demographic characteristics, TACS, CACS, and echocardiographic variables according to LVH and TACS are shown in Table 1. There were 171 patients with no LVH and low TACS, 73 patients with LVH and low TACS, 168 patients with no LVH with high TACS, and 75 patients with LVH and high TACS.
Table 1
Patient characteristics

Values are presented as mean±standard deviation, median (range), or number of patients (%).
ANOVA = analysis of variance; BMI = body mass index; CACS = coronary artery calcium score; CT = computed tomography; E/e' = the ratio of early diastolic mitral inflow to mitral annular velocity; HDL = high density lipoprotein; LDL = low density lipoprotein; LVEDD = left ventricular end-diastolic dimension; LVEF = left ventricular ejection fraction; LVESD = left ventricular end-systolic dimension; LVH = left ventricular hypertrophy; LVMI = left ventricular mass index; TACS = thoracic aorta calcium score.
*p values were calculated by ANOVA for continuous variables and by χ2 test for categorical variables.
![]()
Table 2 reports resting and peak exercise SBP and PP values, as well as the Δ in both parameters, according to the presence of LVH and median value threshold of TACS. Resting SBP (128±17 mmHg vs. 124±16 mmHg, p=0.003) and PP (51±15 mmHg vs. 48±14 mmHg, p=0.022) were higher in those with LVH, although the ΔSBP (51±22 mmHg vs. 52±24 mmHg, p=0.631) and ΔPP (51±24 mmHg vs. 52±22 mmHg, p=0.720) were not very dissimilar between LVH groups. The high TACS group demonstrated a somewhat higher ΔSBP (54±23 mmHg vs. 50±23 mmHg, p=0.045) and ΔPP (54±24 mmHg vs. 49±22 mmHg, p=0.031), while resting SBP (127±17 mmHg vs. 123±15 mmHg, p=0.006) and resting PP (51±15 mmHg vs. 47±13 mmHg, p=0.003) also exhibited similarly elevated levels compared with the low TACS group.
Table 2
Blood and PP changes based on LVH and TACSs

Values are presented as mean±standard deviation.
LVH = left ventricular hypertrophy; PP = pulse pressure; SBP = systolic blood pressure; TACS = thoracic aorta calcium score; ΔPP = difference in pulse pressure between rest and peak exercise; ΔSBP = difference between systolic blood pressure at rest and peak exercise.
![]()
Over a median follow-up period of 65 months (IQR, 17–89 months), there were 39 composite events (8.0%) including 2 cardiac deaths (0.4%), 12 inpatient admissions for heart failure (2.5%), 9 obstructive CADs requiring coronary intervention (1.8%), and 16 strokes (3.3%). In Table 3, univariate Cox regression analysis revealed that age (HR, 2.93; 95% CI, 1.33–6.42; p=0.007) and high TACS (HR, 2.34; 95% CI, 1.19–4.84; p=0.015) were significant predictors of the composite study endpoint. Further, in Table 4, multivariate Cox regression analysis found LVH to be an independent predictor (HR, 2.41; 95% CI, 1.19–4.90; p= 0.015) of the composite study endpoint, even after adjusting for age, gender, hypertension, diabetes mellitus, and BMI. High TACS was also an independent predictor (HR, 2.09; 95% CI, 1.01–4.32; p=0.048) for study endpoint, even after adjusting for clinical variables. Notably, when patients were stratified according to the presence or absence of LVH and TACS, those with LVH and high TACS were at greater risk (HR, 4.51; 95% CI, 1.71–11.88; p=0.002) of experiencing the composite study endpoint, regardless of age, gender, hypertension, diabetes mellitus, and BMI (Table 4). The other strata of LVH and TACS did not have significant predictors for the composite study endpoint (p>0.050, all).
Table 3
Univariate HRs for predicting composite study endpoints
BMI = body mass index; CACS = coronary artery calcium score; CI = confidence interval; HR = hazard ratio; LVH = left ventricular hypertrophy; TACS = thoracic aorta calcium score.
![]()
Table 4
Multivariate HRs for predicting composite study endpoints

BMI = body mass index; CI = confidence interval; HR = hazard ratio; LVH = left ventricular hypertrophy; TACS = thoracic aorta calcium score.
![]()
Figure 2 displays Kaplan-Meier survival curves for time-to-event stratified by LVH and TACS groups. In particular, among patients with LVH, the concurrent presence of a high TACS was associated with an unfavorable event-free survival (log-rank p=0.039), whereas for individuals without LVH, time to events did not differ for those with either a high or low TACS (log-rank p=0.109). When the patients were divided based on the presence of LVH, LVH was not found to be associated with significant prognostic markers in patients with low TACS (log-rank p=0.783), while LVH demonstrated borderline significance for predicting poor prognosis for those with high TACS (log-rank p=0.099).
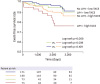 | Figure 2Kaplan-Meier survival curves displaying time-to-event rates stratified according to LVH and TACS.
LVH = left ventricular hypertrophy; TACS = thoracic aorta calcium score.
|
The ICC for intraobserver reproducibility was 0.999 (95% CI, 0.998–0.999) for TACS in non-contrast CT scan, suggesting excellent correlation.
DISCUSSION
The principal finding of this study was that TACS is a robust predictor for a composite of cardiovascular events and cardiac death in older-aged individuals with LVH, whereas the prognostic role of TACS independent of LVH was less pronounced; the latter might indicate a relatively healthy myocardium without structural impairment. To our knowledge, this is the first study to document the differential prognostic utility of TACS based on the vulnerability of individual myocardial properties.
LVH is frequently found in hypertensive patients and results from complex interactions among several hemodymic and non-hemodynamic components.5) LVH usually occurs in response to hemodynamic overload in some physiological and pathological conditions. Hypertrophic growth of cardiomyocytes is a key mechanism of LVH, by which the heart reduces the LV wall and stress is caused by systemic pressure overload.13) In addition to increased afterload with high blood pressure, other elements such as ethnicity, gender, environmental influences, obesity, as well as neurohumoral and genetic considerations could affect the LV mass.14)15)16) Secretion of vasoactive peptides can increase during LVH and can significantly impact LVH caused by high blood pressure. Although antihypertensive treatments can reduce blood pressure levels in hypertensive patients, it has been reported that this approach is not always useful for delaying or preventing LVH.17) LVH leads to an increased myocardial mass/volume ratio, and the degree of hypertrophy is associated with chamber stiffness. Fibrillar collagen, as well as cardiomyocyte hypertrophy, accumulates in the extracellular space and the reactive and progressive interstitial, and perivascular fibrosis accounts for abnormal myocardial stiffness in LVH and, ultimately, LV systolic and diastolic dysfunction.18)
Aortic stiffness is associated with diastolic dysfunction in patients with early stage hypertension or diabetes mellitus, which suggests a common pathophysiological link between aortic stiffness and LV diastolic function, irrespective of LVH.19)20) We previously reported on the association between heavy aortic calcification and arterial stiffening in elderly male patients with hypertension and subsequently propose that the role of aortic calcification might reflect a simple imaging surrogate of aortic stiffness.9) In this study, we found that patients with LVH and a high TACS experienced the poorest clinical outcomes compared with the other subgroups, including those without LVH and those with LVH and low TACS (though TACS values did not differ between LVH groups). Therefore, based on these results, the impact of aortic calcification on adverse clinical outcomes might be more prominent in patients with LVH, despite similarities in the total amount of aortic calcium deposits in those with and without LVH.
This finding could be caused by diseased myocardium such as LVH, which is more easily influenced by afterload increase associated with aortic stiffness. A similar exaggerated systolic load interaction has been documented in patients that present with heart failure and preserved systolic function. Moreover, aortic stiffness can potentially exacerbate LV systolic load interaction with diastolic function, and this ventricular-systolic and arterial stiffening might further exacerbate blood pressure lability and diastolic dysfunction under stress, which is often present in patients with heart failure and preserved systolic function.21) Undoubtedly, further studies are needed to evaluate the impact of high TACS on clinical outcomes, as well as LVH progression and diastolic function, in various diseases that involve the myocardium, such as heart failure and cardiomyopathies. In addition, further investigation is required to identify an approach for combining LVH and TACS to efficiently predict cardiovascular outcomes.
In contrast to the current study, Kim et al.22) demonstrated that, in the presence of CACS=0, measurement of TACS is unlikely to provide sufficient additional prognostic information to further improve risk assessment. The differential prognostic impact would be caused by the difference in aortic calcium burdens between the study populations. We previously demonstrated that the conflicting data on the prognostic role of aorta calcification resulted from the amounts of calcium deposited in the aortic wall, and that heavy aortic calcification would be required to cause remarkable changes in arterial stiffness with vascular calcification.23) In this study, we found that those with low TACS showed relatively low CACS (median of 0) value. Therefore, the presence of CACS=0 might suggest that thoracic aortic calcium burden is also too low to modify arterial stiffness and clinical outcomes. Consequently, low CACS, which reflects relatively low TACS in the population, would not alter vascular stiffness or clinical outcomes.
In this study, resting SBP and PP were higher in the LVH group compared with the no LVH group, although the ΔSBP and ΔPP did not differ between those with or without LVH. Of note, when subjects were divided into 2 categories on the background of low or high TACS, both resting and peak exercise hemodynamic variables demonstrated clear differences between the low and high TACS groups. Based on this result, it is possible that a potential mechanism mediates unfavorable clinical outcomes in patients with high TACS and could be associated with the dynamic rise of SBP and the widening of PP during exercise; however, additional studies are necessary to support this hypothesis.
The current findings were based on a retrospective analysis, which limits this study from inferring a causal relationship between TACS or CACS and the composite endpoint. Despite this, we carefully reviewed all medical records and CT images in an effort to avoid possible biases. Arterial stiffness was not measured, and follow-up echocardiography data were not obtained. Hence, the current study was unable to confirm whether arterial stiffness and/or high aortic calcification might have aggravated the progression of LVH. Further studies with concurrent measures of arterial stiffness, aortic calcification, and serial echocardiography are warranted to support this conclusion. Although we excluded patients with myocardial disease, such as hypertrophic cardiomyopathy or infiltrative cardiomyopathy, it can be difficult to differentiate early stages of diffuse type hypertrophic cardiomyopathy from LVH in patients with a hypertensive heart condition. Therefore, the cause of LVH in some of the patients remains unclear, although other risk factors such as ethnicity, gender, environmental influences, obesity, and neurohumoral and genetic factors might affect LV mass. Traditional cardiovascular risk factors for cardiovascular outcomes, such as hypertension and diabetes mellitus, were not risk factors for outcomes in the current study. We excluded patients with obstructive CAD who were at high risk for future cardiovascular events related to ischemic heart disease, and the exclusion of these high-risk populations of CAD might have resulted in the lack of association with traditional CAD risk factors. Therefore, it is difficult to distinguish ascending aortic root calcification from aortic valve calcification. For better diagnostic accuracy, we rechecked the use of reformatted sagittal and coronal planes in cases where the differentiation between aorta and valve calcification was difficult, based on axial images. Although different prognostic roles between intimal and medial calcification are important issues related to aortic calcification, we could not differentiate intimal calcification from medial calcification. Unfortunately, because there is not currently a method for differentiating intimal calcification from medial calcification in intact aorta (without dissection) by CT imaging or by other non-invasive imaging modalities, further studies are required to find a novel method for localizing vascular calcification. Inclusion of the entire chest wall is necessary to assess TACS from coronary calcium scan. Although this might raise questions about the full field of view, this approach is advantageous for early detection of lung cancer and other lung diseases.24) Furthermore, the radiation dose in our study was too low for a calcium scan, even with a full field of view (mean value of 1.5 mSv). We cannot discount the possibility that the number of events in the current study might have been underreported, as we relied primarily on gathering events data from hospital reports. Nevertheless, such underestimation of events would likely have been mitigated by a comparable underestimation across all groups.
In this study, the prognostic impact of TACS was different between patients with LVH and those without LVH. TACS provided a robust diagnostic approach for a composite of cardiovascular events in older-aged individuals with LVH. The findings were less pronounced in those with relatively healthy myocardium, as demonstrated by the absence of LVH. The impact of TACS, which might translate into afterload increase, should be accounted for when attempting to offset the progression of disease, especially in patients with established LVH.
 XML Download
XML Download