

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia, occurring in 1–2% of the general population, and its occurrence has increased rapidly in Korea.1)2) It is associated with a 5-fold increase in stroke risk, and one in 5 cases of stroke is attributed to this arrhythmia.3) Oral anticoagulant (OAC) treatment can prevent the majority of ischemic strokes in patients with AF and prolong life.4) It is superior to no treatment or aspirin in patients with different profiles for stroke risk.5) Non-vitamin K antagonist oral anticoagulants (NOACs) can have a considerable effect on standard stroke prevention and management in AF. Their predictable pharmacodynamics and kinetics as well as fewer drug-drug and drug-food interactions than those of warfarin can simplify their use by healthcare professionals and patients. Several major trials have shown that NOACs have on-par or better efficacy and safety than warfarin.6)7)8)9)
Regulatory approvals of NOACs were based on 4 large randomized phase III trials evaluating dabigatran (Pradaxa®; Boehringer Ingelheim Pharmaceuticals, Inc., Ridgefield, CT, USA), rivaroxaban (Xarelto®; Janssen Pharmaceuticals, Inc., Titusville, NJ, USA), apixaban (Eliquis®; Bristol-Myers Squibb Company, Princeton, NJ, USA), or edoxaban (Savaysa®; Daiichi Sankyo, Inc., Parsippany, NJ, USA) vs. warfarin (Coumadin®; Bristol-Myers Squibb Company) for AF.6)7)8)9) The results of the trials showed that all NOACs were at least non-inferior to warfarin in prevention of stroke/thromboembolism (TE). Intracranial bleeding was a safety outcome in the trials, and all NOACs were associated with lower rates of intracranial bleeding than was warfarin. However, the trials were designed differently, with variations in the inclusion/exclusion criteria and either one dose or a low/high dose of the NOAC drug. Some of these differences have challenged the ability to directly compare stroke/TE prophylaxis and risk of intracranial bleeding with dabigatran, rivaroxaban, or apixaban relative to warfarin. Importantly, results of randomized controlled trials are wholly convincing, but comparative data on effectiveness and intracranial bleeding are sparse in real-world patients. Recently, a considerable amount of real-world data on NOACs has been published (Table 1). Real-world data are complementary to those obtained from large randomized phase III trials, providing new information on the “real-world” absolute risks of ischemic and hemorrhagic stroke with NOACs vs. vitamin K antagonists (VKAs). Moreover, real-world fragile patients might have been included (e.g., patients with increased risk of bleeding, liver disease, and chronic kidney disease), although these patients would be less represented in the trials.10) This paper highlights recently published real-world data of NOACs and further recommends NOAC dosages for Korean patients.
Table 1
Comparison of NOACs

| Author | Study design | Region | Enrollment period | Cohort size | Endpoints | NOACs analyzed |
|---|---|---|---|---|---|---|
| Laliberté et al.30) | RC | US | May 2011 to Jul 2012 | 30,479 | Effectiveness and bleeding | R vs. D |
| Bouillon et al.31) | RC | France | Jan 2011 to Nov 2012 | 17,410 | Effectiveness and bleeding | D, R, or W |
| Abraham et al.32) | RC | US | Nov 2010 to Sep 2013 | 219,027 | GI bleeding | D, R, or W |
| Maura et al.33) | RC | France | Jul to Nov 2012 | 32,807 | Effectiveness and bleeding | D, R, or W |
| Graham et al.17) | RC | US | Nov 2011 to Jun 2014 | 118,891 | Stroke, bleeding, and mortality | R vs. D |
| Noseworthy et al.11) | RC | US | Oct 2010 to Feb 2015 | 31,574 | Effectiveness and bleeding | D, R, or W |
| Deitelzweig et al.34) | RC | US | Jan 2012 to Mar 2014 | 74,730 | Bleeding-related hospital readmissions | D, R, or W |
| Coleman et al.35) | RC | US | Jan 2012 to Oct 2014 | 38,831 | Stroke, ICH | A, R, or W |
| Lip et al.36) | RC | US | Jan 2012 to Dec 2013 | 29,338 | Bleeding | A, D, R, or W |
| Halvorsen et al.37) | Registry | Norway | Jan 2013 to Jun 2015 | 32,675 | Bleeding | A, D, R, or W |
| Chan et al.15) | RC | Taiwan | Feb 2013 to Dec 2013 | 304,252 | Effectiveness and bleeding | D, R, or W |
| Larsen et al.12) | RC | Denmark | Aug 2011 to Oct 2015 | 61,678 | Effectiveness and bleeding | A, D, R, or W |
| Yao et al.38) | RC | US | Oct 2010 to Jun 2015 | 125,243 | Effectiveness and bleeding | A, D, R, or W |
| Lip et al.39) | RC | US | Jan 2012 to Dec 2014 | 33,262 | Major bleeding | A, D, R, or W |
| Gorst-Rasmussen et al.16) | Registry | Denmark | Feb 2012 to Jul 2014 | 22,358 | Effectiveness and bleeding | D, R, or W |
| Staerk et al.13) | Registry | Denmark | Aug 2011 to Dec 2015 | 54,312 | Effectiveness and ICH | A, D, R, or W |
| Lamberts et al.22) | Registry | Denmark | Aug 2011 to Dec 2015 | 54,312 | Bleeding and non-persistence | A, D, R, or W |
| Hohnloser et al.40) | Registry | Germany | Jan 2013 to Mar 2015 | 35,013 | Bleeding | A, D, R, or W |
| Hernandez and Zhang18) | RC | US | Nov 2011 to Dec 2013 | 17,507 | Effectiveness and bleeding | R vs. D |
REAL-WORLD NOAC DATA: STROKE AND TE
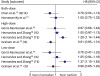
In cohorts of patients with non-valvular AF drawn from a large US database of commercial and Medicare supplement claims, dabigatran, rivaroxaban, and apixaban appeared to have similar effectiveness.11) In Danish nationwide registries, all NOACs appeared to be safe and effective alternatives to warfarin in a routine care setting.12) Recently, Staerk et al.13) reported that, in anticoagulant-naïve patients with AF, treatment with dabigatran, rivaroxaban, and apixaban was not associated with a significantly lower risk of stroke/TE than in patients administered anticoagulants (Figure 1).
Figure 1
Comparison of each NOAC and warfarin in risk of stroke/TE in patients with AF.
AF = atrial fibrillation; CI = confidence interval; HR = hazard ratio; NOAC = non-vitamin K antagonist oral anticoagulant; TE = thromboembolism.

In a recent systematic review and meta-analysis, rivaroxaban was as effective as dabigatran, but was more effective than warfarin for the prevention of stroke/TE in patients with AF.14) Rivaroxaban was associated with a similar risk of stroke/TE to dabigatran11)15)16)17)18) (hazard ratio [HR], 1.02; 95% confidence interval [CI], 0.91–1.13; I2=70.2%, n=5), with a pooled rate for rivaroxaban at 0.3%/year vs. dabigatran at 0.3%/year (Figure 2).14) Noseworthy et al.11) reported that apixaban was as effective as rivaroxaban and dabigatran in the prevention of stroke/systemic embolism in patients with AF.
REAL-WORLD NOAC DATA: BLEEDING
Each NOAC compared with warfarin in risk of major bleeding in patients with AF
Figure 3 shows the comparison of each NOAC with warfarin in risk of major bleeding in patients with AF. In the real-world study with elderly Medicare users of dabigatran,19) at the 150 mg twice-daily dose, the risk of intracranial bleeding and mortality in patients aged ≥65 was significantly reduced compared with that of warfarin. Similar observations were shown in real-world studies with elderly patients from other countries such as Canada.20) Carmo et al.21) published a meta-analysis of several observational trials of dabigatran. In total, 210,279 and 510,019 patients treated with dabigatran and warfarin, respectively, were included in the meta-analysis, which showed significant difference in mortality, intracranial hemorrhage, and major bleeding, in favor of dabigatran. Subgroup analysis showed greater benefits in the prevention of ischemic stroke with dabigatran than with warfarin in the elderly, but there was no significant benefit over warfarin for major bleeding related to age. The increased evidence of gastrointestinal bleeding with dabigatran 150 mg twice daily was in line with the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) trial, whereas dabigatran 110 mg twice daily showed no difference in gastrointestinal bleeding from warfarin.
Figure 3
Comparison of each NOAC and warfarin in risk of major bleeding in patients with AF.
AB = any bleeding; AF = atrial fibrillation; CI = confidence interval; HR = hazard ratio; ICH = intracranial hemorrhage; NOAC = non-vitamin K antagonist oral anticoagulant.

In Danish nationwide registries, both apixaban and dabigatran had significantly lower risks of death, any bleeding, or major bleeding than did warfarin.12)13) In patients with high stroke and bleeding risks, dabigatran was the only NOAC associated with persistence of a significant low risk of intracranial bleeding. Another study showed that apixaban had a lower adjusted major bleeding risk than those of rivaroxaban, dabigatran, and warfarin.22)
However, rivaroxaban was comparable to warfarin in major bleeding incidences, with an increased risk of gastrointestinal bleeding and decreased risk of intracranial hemorrhage.14)
Comparison of NOACs in risk of major bleeding in patients with AF
Figure 4 shows the comparison of NOACs in risk of major bleeding in patients with AF. In a recent systematic review and meta-analysis, the major bleeding risk was significantly higher with rivaroxaban than it was with dabigatran (Figure 4A) or apixaban (Figure 4B), as were all-cause mortality and gastrointestinal bleeding. Rivaroxaban was associated with increased risk of all-cause mortality15)16)17)18) (HR, 1.23; 95% CI, 1.12–1.33), any bleeding16)17)18) (HR, 1.33; 95% CI, 1.17–1.49), and gastrointestinal bleeding15)17)18) (HR, 1.33; 95% CI, 1.18–1.48), but with similar risk of acute myocardial infarction15)17) (HR, 0.81; 95% CI, 0.43–1.19) and intracranial hemorrhage11)15)17)18) (HR, 1.22; 95% CI, 0.85–1.59) compared with dabigatran. Apixaban was comparable to dabigatran in major bleeding (Figure 4C).

REAL-WORLD DATA FOR THE REDUCED DOSAGE OF NOAC
While NOACs do not require the meticulous dose adjustments required for warfarin, a clinical evaluation of appropriate (constant) doses is still necessary. A significant minority (approximately 1 in 8) of US patients in the community received NOAC doses inconsistent with labeling. NOAC over- and under-dosing are associated with an increased risk for adverse events.23) The efficacy and safety of reduced NOAC doses were reported in several studies. Recently, Nielsen et al.24) reported that, in the propensity weighted Danish nationwide study of reduced-dose NOAC regimens, apixaban 2.5 mg twice a day was associated with an increasing trend of ischemic stroke/systemic embolism rates compared with warfarin, while rivaroxaban 15 mg once a day and dabigatran 110 mg twice a day showed a trend of lower thromboembolic rates. The results were not significantly different. Rates of bleeding (the principal safety outcome) were significantly lower for dabigatran than for other agents, but did not significantly differ for apixaban and rivaroxaban compared with warfarin. Because the efficacy and safety were changed by reducing the dosage of NOAC, strict adherence to the dose reduction guideline is necessary.
Varying degrees of renal function require recommendations for reduced dosing regimens of these drugs; however, different cut-off values for age, body weight, or interacting drugs also require consideration for appropriate dose selection.25) Indeed, both age and chronic kidney disease in patients with AF intensify the risk of stroke and increase the risk of bleeding during antithrombotic treatment.26) In routine clinical practice, prescribed NOAC doses are often inconsistent with drug labeling. These prescribing patterns might be associated with worse safety profiles with no benefit in effectiveness in patients with severe kidney disease and worse effectiveness with no benefit in safety in apixaban-treated patients with normal or mildly impaired renal function.27)
RECOMMENDATION OF DOSE REGIMEN FOR KOREAN PATIENTS
Elderly patients with AF (such as those aged ≥80 years) and patients with impaired renal function were included in the landmark trials of NOACs, but these important subgroups comprised only a small proportion of the patient populations. For dabigatran, reduction of the daily recommended dose to 110 mg twice daily is indicated for patients aged ≥80 years. This dose can be reduced to 110 mg twice daily if the patient is aged 75–79 years and has other comorbidities that could affect bleeding risk such as previous gastritis, peptic ulcer disease, and moderate renal impairment. Indeed, label (or guideline) adherent use of dabigatran is clearly associated with better outcomes for stroke, major bleeding, and mortality.28)29) Insufficient published data for apixaban, edoxaban, and rivaroxaban indicate that further work is needed to clarify the bleeding risks of these NOACs in the elderly.
For Korean patients with AF, a reduced dosing regimen for dabigatran (110 mg twice a day) in patients aged ≥80 years or who have an estimated glomerular filtration rate (eGFR) of 30–50 mL/min; rivaroxaban (15 mg once daily) in patients aged ≥80 years or with an eGFR of 15–49 mL/min; apixaban (2.5 mg twice a day) if 2 of the 3 following criteria are present: age ≥80 years or an eGFR 15–29 mL/min or body weight ≤60 kg; or edoxaban (30 mg once daily) if eGFR is 15–50 mL/min are recommended (Table 2).
Table 2
Dose reduction of NOACs

CONCLUSION
Real-world data is complementary to large randomized phase III trials by providing new information on the real-world absolute risks of ischemic and hemorrhagic stroke with NOACs vs. VKA. This paper highlighted recently published real-world data of NOACs and further recommended dosages for NOACs for Korean patients.
 XML Download
XML Download