

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Right ventricular outflow tract reconstruction with a homograft conduit has been widely used for over 30 years.1) Congenital heart disease with pulmonary atresia and truncus arteriosus are typical diseases that require a homograft conduit at an early age. The short-term results of homograft conduits are excellent, but stenosis is both an inevitable outcome and the primary indication for subsequent surgical re-intervention.2)3) This stenosis, exacerbated by calcification, might be accelerated in the pediatric population despite various preservation techniques.4)5) Although the most effective alternate palliation is conduit replacement, there have been various efforts to reduce the risk associated with repetitive replacements, such as balloon dilatation, stent implantation, and percutaneous pulmonary valve implantation.6)7)8)9)10)11)12) The effect of balloon dilatation of homografts in the pulmonary position in congenital heart disease is controversial due to the difficulty in defining efficacy and the small size of published studies. Some studies have reported that balloon dilatation fails to prolong homograft life and recommend abandoning balloon dilation of homograft conduits.2)3)6)13) However, recent retrospective studies have concluded that balloon dilatation of homograft conduits in the pulmonary position has a favorable effect.7)8) Balloon dilatation of homografts in children or adolescents can postpone surgical valve or percutaneous valve implantation by 1 or 2 years, reducing the overall number of valve replacements needed. Accordingly, we retrospectively reviewed our experience to determine whether balloon dilatation is associated with postponement of conduit replacement.
SUBJECTS AND METHODS
We retrospectively reviewed the medical records of all patients who underwent balloon dilatation of a homograft in the pulmonary position at Samsung Medical Center or Sejong General Hospital from January 2001 to December 2015. Patients with medical records lacking hemodynamic data or without follow-up were excluded. Patient demographics, cardiac diagnoses, catheter intervention records (including hemodynamic data), and surgical records were obtained. The time of homograft conduit insertion, balloon dilatation, and subsequent intervention such as balloon dilatation, stent insertion, or conduit change were recorded, and the intervals between each event were calculated.
The decision for cardiac catheterization was based on echocardiographic evaluation and the patient's clinical condition. Balloon dilatation was performed by a cardiac interventionist specializing in congenital heart disease, and the decision to perform the procedure was based not only on pressure differences through homograft conduit stenosis and right ventricular pressure compared to descending aortic pressure, but also on the degree of calcification. A conventional balloon was chosen by the interventionist according to the conduit size described in the surgical record. A double balloon technique was chosen when the available balloon was limited. A standard balloon angioplasty technique was used as described previously,14)15) and pressures before and after balloon dilatation were measured.
Two-dimensional (2D) echocardiography was performed the day after the procedure, and routine echocardiographic follow-up was maintained after discharge. Future interventions were decided after discussion with surgeons. The last follow-up date was the date of the following intervention or the last hospital visit.
We arbitrarily defined a favorable result after balloon dilatation as postponement of the next intervention to 24 months or later and investigated differences between patients divided according to time to next intervention (less than 24 months vs. greater than 24 months).
Statistical analyses were performed using SPSS 23.0 (IBM Corp., Armonk, NY, USA). The mean, median, standard deviation, and range were calculated for continuous variables. Frequencies were calculated for nominal variables. Changes after balloon dilatation were compared with the Wilcoxon signed rank test. Kaplan-Meier curves were used to analyze freedom from re-intervention. Cox proportional hazard model was used to identify risk factors for early re-intervention. The log-rank method was used to compare Kaplan-Meier curves of the 2 groups. The time to the following intervention was compared using the Mann-Whitney U test. Values of p<0.050 were considered statistically significant. The institutional review board approved this study, and the requirement for consent from patients or parents was waived.
RESULTS
Twenty-eight balloon dilatations were performed in 26 patients, 16 of whom were male. The original diagnoses included pulmonary atresia/ventricular septal defect (n=9), truncus arteriosus (n=5), Ross operation (n=6), tetralogy of Fallot (n=3), transposition of the great arteries/pulmonary stenosis (n=3), pulmonary atresia without ventricular septal defect (n=1), and congenitally corrected transposition of the great arteries/pulmonary stenosis (n=1). The origins of the homograft were the aorta (n=15), pulmonary artery (n=9), and femoral vein (n=4). The median ages at conduit insertion and balloon dilatation were 20.3 (0.4–557.0) months and 4.5 (0.6–53.3) years, respectively. The median interval from conduit insertion to balloon dilatation was 26.7 (3.3–137.4) months, and the interval to next intervention from balloon dilatation was 12.9 (0.1–100.0) months. Conduit size ranged from 9 mm to 25 mm (median 15 mm). The median follow-up period after balloon dilatation was 12.6 months, and subsequent intervention such as surgical or balloon intervention was confirmed in 25 cases.
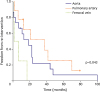
A second trial was performed in 2 patients, and a double balloon was used in 1 trial. There was 1 case of balloon rupture in 1 trial, but there were no serious complications. The hemodynamic data before and after balloon dilatation are summarized in Table 1. The pressure difference through the stenotic conduit and the ratio of right ventricle to aorta pressure were both significantly improved after balloon dilatation (p<0.001). The median period of freedom from re-intervention was 16.6 months (Figure 1). Cox regression analysis showed that homograft type was a unique risk factor of decreased period of freedom from re-intervention (Table 2). However, pressure differences, right ventricle pressure ratio, balloon size to conduit diameter ratio, interval from homograft insertion, and conduit size were not significant risk factors. The median period of freedom from re-intervention was 37.6 months for pulmonary artery homografts, 18.7 months for aorta homografts, and 1.3 months for femoral vein homografts (p=0.043) (Figure 2).
Table 1
Patient characteristics according to balloon dilatation of homografts

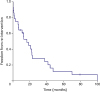
Table 2
Relative risk by Cox proportional hazards model

Figure 2
Differences in freedom from re-intervention according to type of homograft; aorta, pulmonary artery and femoral vein.
In cases of favorable result after balloon dilatation as defined above, the pressure ratio of the right ventricle to the aorta before balloon dilatation was significantly lower than in other cases. Age of conduit operation, interval from conduit surgery to balloon dilatation, pressure difference before balloon dilatation, and size ratio of balloon to conduit were not different between patients with favorable results and other patients (Table 3).
Table 3
Differences in patients who received re-intervention after balloon dilatation based on a 24-month re-intervention threshold

DISCUSSION
Based on our findings, balloon dilatation of homograft conduits in the pulmonary position led to postponement of valve replacement, with the greatest benefit seen with pulmonary artery homografts. While the interval in some cases was small, reducing the number of repetitive cardiac surgeries or postponing a subsequent surgery is a worthwhile goal, especially for pediatric patients, because surgical conduit revision is associated with increased risk of mortality.16) Percutaneous pulmonary valve implantation represents a possible alternative, but is not currently available in many areas.
Sanatani et al.6) concluded that balloon dilatation of homograft conduits is not recommended due to the very limited and only transient benefit observed in a small series of patients. However, despite the small number of patients in their study, the next operation was postponed in a majority of patients. The transient effect of balloon dilatation reported in their study was verified by echocardiography; however, pressures measured by Doppler and catheterization can differ significantly. It is also important to note that the majority of conduits in their study were aortic homografts; however, pulmonary homografts are known to last longer than aortic homografts.4)5)17)18)19) Consistently, we found that balloon dilatation in pulmonary homografts provided better results than aortic or femoral vein homografts, although the reasons behind these differences are not entirely clear. Bertels et al.7) reported favorable effects after balloon dilatation of homografts, but could not identify any significant factors predictive of a favorable effect. Powell et al.10) proposed that absence of calcification and younger conduit age are factors associated with better results. While our definition of a 24-month delay to re-intervention after ballooning as a favorable result was both subjective and arbitrary, a total of one-third of our patients met this criteria. Thus, we considered it meaningful to compare patients with favorable results to other patients. The group with favorable results after balloon dilatation had a longer interval from conduit insertion, although the difference was not significant (27.0 months vs. 22.3 months), which was similar to Bertels et al.'s findings.7) We also did not evaluate calcification in our study, as this parameter is difficult to quantify.
In cases of bioprosthetic valves in the pulmonary position, balloons with the same diameter as the valve are recommended for dilatation.15) Balloon size compared to conduit size was not a factor associated with good outcomes in our study, consistent with the results of previous studies.6)7)20) Balloon pressure rather than balloon size might be important, because good results have been reported with ultra-noncompliant balloons for angioplasty of homografts.8) We used both high pressure and conventional balloons because of limited availability. Specifically, we were concerned about conduit rupture in cases with high pressure or using large balloons based on case reports of conduit rupture requiring urgent surgery.7)8)
Based on length of time to the next intervention after balloon dilatation, femoral vein homografts were associated with the worst outcomes in our study. The reasons for this result are not clear, but femoral vein homografts tended to be used in small patients because of the smaller size of the homografts. Rapid somatic growth in patients compared to static conduits and subsequent rapid calcification could also explain the worse outcomes associated with femoral vein homograft.
Relatively early balloon dilatation at a lower right ventricular pressure compared to systemic pressure was an important factor for better outcome, defined as delayed re-intervention in our study. Although the difference did not reach the level of significance, the pressure gradient over conduits was also lower in the patient group with a good outcome. Due to different clinical objectives for each case, our criteria (postponement of 24 months) should be considered as only one possible outcome. However, the period of freedom from re-intervention in this study was similar to that of another study.7)
There were several limitations to this study. First, a retrospective review does not have the statistical strength of a randomized control study. In addition, the indications for balloon dilatation were not applied uniformly to all patients with homograft conduits. Based on our standard practice, a maximal pressure gradient over the conduit greater than 50 mmHg was an indication for catheterization, while a similar pressure gradient or a ratio of right ventricle to aorta pressure greater than 0.65 was used as an indication for balloon dilatation.21) However, it was the interventionist who ultimately decided on balloon dilatation in each case after considering not only hemodynamic data, but also the degree of calcification and conduit size compared to somatic size, among other criteria. Another limitation of this study was that the time to re-intervention could have been biased by previous interventions other than those used as indications for intervention. We also did not document the impact on pulmonary regurgitation after balloon dilatation because it was difficult to quantify the amount of regurgitation in cases of severe stenosis. Right ventricular function was not evaluated for the same reason. Finally, the small number of patients in our study made it challenging to draw conclusions about the effect of balloon dilatation on postponing valve replacement. In the future, well controlled studies comprising a larger patient series will be useful for determining the optimal timing for balloon dilatation of homograft conduits in the pulmonary position.
In conclusion, based on our retrospective analysis of a small series of patients, balloon dilatation of homograft conduits in the pulmonary position appeared safe and had a limited effect on postponement of the next re-intervention. The longest delays to re-intervention occurred with pulmonary homografts, and a relatively lower right ventricle/aorta pressure ratio was associated with a better outcome, as defined by postponement of the next re-intervention.
 XML Download
XML Download