

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Recently, minimally invasive surgical (MIS) approaches have been more widely adopted in cardiothoracic surgery, including congenital heart surgery. A limited sternotomy or modified sternotomy has been tried, but a midline scar cannot be avoided.1)2)3)4) Right anterolateral thoracotomy or right vertical thoracotomy has also been applied, but they require a relatively large incision for the operation using thoracotomy only, and postoperative pain was universal and intense.5)6)7) Excellent success rates and low complication rates in atrial septal defect (ASD) closure have been reported with thoracoscopic surgery supported by the robotic Da Vinci system.8)9)10) However, the Da Vinci system needs expensive equipment and complex technical assistance. The aim of this study was to evaluate our single-center experience and the mid-term results of thoracoscopic ASD closure without robotic assistance.
SUBJECTS AND METHODS
Study population
From June 2006 to July 2014, 67 patients with ASD underwent thoracoscopic ASD closure at our institute. Indications were 1) a weight of 30 kg or more, 2) no prior operation on the right chest, 3) no history of chronic lung disease, and 4) no more than moderate pulmonary hypertension on preoperative echocardiography. One patient who required intraoperative sternotomy conversion was excluded. Sixty-six patients were finally reviewed. The study protocol was approved by the Samsung Medical Center Institutional Review Board, which waived the need for patient consent.
Operative procedures
Under general anesthesia, double-lumen endotracheal intubation was performed for selective left pulmonary ventilation. Trans-esophageal echocardiography was inserted and an external defibrillator patch was attached. Prior to the operation, a heparin-infused venous cannula (Medtronic Bio-Medicus Inc., Eden Prairie, MN, USA; 14–17 Fr.) was inserted into the superior vena cava (SVC) by the anesthesiologist. When the patient was supine with the right chest elevated 30 degrees, a small incision was made along the inframammary groove and a 5-mm thoracoscope was inserted into the 4th intercostal space (ICS). The pleural cavity was examined to assess the existence of adhesions and anatomical relationships. A working window was made by extending the prior incision 4 to 5 cm (Figure 1). For cardiopulmonary bypass (CPB), a 2- to 3-cm oblique incision was made in the right inguinal area and the right femoral artery and vein were identified. A 5-mm camera port was made in the 6th ICS. The port for the aortic cross clamp (ACC) was made in the 2nd or 3rd ICS. After systemic heparinization, femoral vein and artery cannulation was performed and CPB was started. The pericardium was harvested at a sufficient distance (>2 cm) from the phrenic nerve. The harvested pericardium was fixed with glutaraldehyde solution. Pericardiotomy was extended up and down. The aorta, the SVC, and the inferior vena cava were exposed. The posterior free edges of the pericardium were suspended under the guidance of the thoracoscope. The SVC was clamped with Glover Bulldog clamps and the inferior vena cava was left open with vacuum-assisted drainage. After a purse-string suture was made at the aortic root, the MiAR™ Aortic Root Cannula (Medtronic Inc., Minneapolis, MN, USA) for cardioplegia infusion was inserted at the aortic root. After a Chitwood clamp (Scanlan International, St. Paul, MN, USA) for ACC was placed on the ascending aorta, the cardioplegia was infused and the aortic root cannula was removed. The ASD was closed directly or with a glutaldehyde-fixed pericardium patch. We mostly performed patch closure. Direct closure was performed in patients with small ASDs or a redundant remnant septum that did not appear to produce tension after direct closure. Before the ASD defect was knotted, de-airing of the left heart was performed with lung inflation. ACC was released after closure of the right atrial incision. The root purse-string suture was tied after de-airing. After weaning from CPB, the femoral vein cannula was removed. Modified ultrafiltration was performed through the femoral artery cannula and the SVC cannula. The SVC cannula was flushed with heparin, clamped, and then removed after the patient was moved to the intensive care unit. A chest tube was placed in the right pleural space from the 2nd ICS port incision and the 6th ICS incision to drain air and effusion.

If the patient had greater than mild-to-moderate tricuspid regurgitation (TR) or mitral regurgitation (MR) preoperatively, we performed tricuspid valve repair (n=8) or mitral valve repair (n=4).
RESULTS
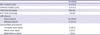
Mean patient age was 27±9 years. The mean ASD size was 25.9±6.3 mm. Eleven patients (16.7%) had a TR pressure gradient that was more than mild-to-moderate. The mean TR pressure gradient was 32.4±8.6 mmHg (Table 1). For ASD closure, 52 (78.8%) patients underwent autologous patch closure and 14 (21.2%) patients underwent primary closure. The mean CPB time was 159±43 minutes and the mean ACC time was 79±29 minutes. Associated procedures and detailed operative data are presented in Table 2. The mean duration of intensive care unit stay was 25±12 hours. The mean ventilator time was 9±5 hours. Blood transfusion was required in 21 (31.8%) patients. There were no early mortalities. There was one wound dehiscence in the ACC port. Two patients required chest tube reinsertion due to pneumothorax after chest tube removal. There were 2 reoperations, one for residual MR of moderate degree after concomitant mitral valve repair, and the other for detachment of the ASD patch. Both reoperations occurred in the early period of our experience. There have been no reoperations in the past 4 years. The mean hospital stay was 6±3 days.
Table 1
Patient characteristics

| Variables | ||
|---|---|---|
| Age (years) | 27±9 | |
| Male sex | 5 (7.6) | |
| ASD size (mm) | 25.9±6.3 | |
| Preoperative TR grade | ||
| Mild to moderate | 8 (12.1) | |
| Moderate | 3 (4.5) | |
| TR pressure gradient (mmHg) | 32.4±8.6 | |
Table 2
Operative procedures
The patient who was excluded from this study because of intraoperative sternotomy conversion was a 29-year-old female who initially underwent thoracoscopic ASD closure. Bleeding occurred from the aortic root cannulation site after ACC release and was uncontrollable despite multiple suture attempts. Finally, we performed a median sternotomy and reconstructed the aortic wall with a homograft patch.
The mean follow-up duration was 33±31 months. Follow-up was completed for 100% of patients. There was no late mortality. Residual ASD, significant TR, and significant MR were not identified on follow-up echocardiography. There was one case of respiratory syncytial virus pneumonia during follow-up. There were no other cardiac-related adverse events including atrial fibrillation, stroke, or reoperations during follow-up.
DISCUSSION
ASD is the most common congenital heart disease in the adult.11) Surgical correction has been successfully performed in most centers recently and postoperative complications, mortalities, and re-interventions are rare.12) Despite improvement in surgical outcomes, a conventional median sternotomy gives rise to cosmetic and psychological problems due to a large scar.
Meanwhile, percutaneous ASD closure has also been performed more actively and widely in recent years.8)9)13)14)15)16)17) Nevertheless, percutaneous ASD closure is hard to apply in primum ASDs, sinus venosus ASDs, large secundum ASDs, ASDs with a small rim that does not allow device fixation, and in patients with multiple fenestrations or atrial septal aneurysms. In addition, surgical backup is required for failure of the intervention. Therefore, these methods can be mutually supportive. In our institution, most patients (n=58, 87.8%) were referred to surgery for an insufficient rim for device closure. Other reasons for referral to thoracoscopic ASD closure are described in Table 3.
Table 3
Reasons for referral to thoracoscopic ASD closure

| No. (%) | |
|---|---|
| Small rim | 58 (87.8) |
| Multiple fenestrations | 2 (3.0) |
| Failure of device closure | 1 (1.5) |
| Patient demand | 5 (7.6) |
To keep up with the improved surgical results and cosmetic demands by patients, a MIS approach has been attempted in ASD closure. Limited sternotomy or modified sternotomy has been applied in the past.1)2)3)4) However, a midline scar results from these techniques and the risk of bleeding or other complications associated with sternotomy cannot be reduced. Right anterolateral thoracotomy or right vertical thoracotomy has also been applied.5)6)7) However, a relatively large incision was required in cases of thoracotomy only, and postoperative pain was universal and intense. Recently, minimally-invasive surgery assisted by the Aesop robotic system and the Da Vinci robotic system has been successfully used for ASD closure.8)9)10)18)19) However, there are significant expenses related to the equipment and support system required. Additionally, the incision scar may be larger than in other techniques because of the relatively large size and number of ports for the robotic arm.
From this viewpoint, thoracoscopic ASD closure has several advantages. It enhances better cosmetic results because of the small number of ports and incisions. Additionally, it does not require expensive equipment or facilities. Successful results of thoracoscopic ASD closure without robotic assistance were reported with excellent early results (no early mortality, no major complications) and no residual shunt during follow-up.20)21) Our study also showed successful early results without early mortality or significant complications except a minor ACC port wound dehiscence. Although there were 2 reoperations, one was for residual MR after concomitant MR repair, which was unrelated to ASD closure, and the other (1.5%) involved reoperation for detachment of the ASD patch. This was comparable to a previous report.22) The mean length of skin incision on the chest was 4.5±0.9 cm and the mean length of the femoral incision was 2.4±0.2 cm. Small postoperative wounds that could be mostly covered by underwear can improve patient satisfaction with regard to psychological and cosmetic aspects (Figure 2).

There may be a concern about the longer CPB time and ACC time than those of ASD closure under conventional sternotomy. Because of the 2-dimensional vision of thoracoscopic surgery, an accurate depth and distance are difficult to achieve and an adaption period might be required. Aortic root bleeding, though very rare, is one of the most catastrophic accidental events in thoracoscopic surgery, and conversion to sternotomy might be required as we mentioned above. After the experience of aortic root bleeding, we released ACC after completion of right atriotomy closure in a double row and weaned CPB after confirming secure hemostasis had been made, especially at the root cannulation site, which needed additional time. However, no serious complications associated with these longer CPB and ACC times were observed in our series.
We believe that patient selection is also important. For the safety of CPB with peripheral cannulation, we did not perform the procedure in patients whose body weight was less than 30 kg. Patients with a moderate or more degree of pulmonary hypertension did not receive this technique. In our series, 92.4% of patients were female (Table 1). Most male patients preferred a sternotomy approach with small skin incision of about 10 cm in length. Anterior thoracotomy incision, although small, could result in a scar on the breast after growth of a young girl whose breasts are not developed yet. On the contrary, incision far from the sub-mammary groove could result in poor cosmetic results also. Dissection beneath the breast tissue may cause asymmetric development of the breast. So, it is our policy to avoid anterior thoracotomy in female patients before puberty. Thoracoscopic ASD closure without robotic assistance can be performed safely with excellent cosmetic results in selected patients. Articulating thoracoscopic equipment or a flexible endoscopic apparatus can improve the surgical field and reduce operative time, and might be applicable in ventricular septal defects or in other heart diseases.
Thoracoscopic ASD closure without robotic assistance is feasible for patients with ASD. This method did not increase surgical risks and provided satisfactory clinical and cosmetic results, suggesting that it is a reliable MIS option for patients with ASD.
 XML Download
XML Download