

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Atrial septal defects (ASDs) are the most common congenital defects in adults following bicuspid aortic valve defects. Prevalence is about 2 per 1,000 live births. ASDs comprise 13% of all congenital defects.1) Morbidity and mortality of ASDs are well documented when left untreated. Percutaneous treatment, which is accepted as the first option today, was first performed just 10 years after surgical treatment methods matured.2) Percutaneous treatment was performed under fluoroscopy for many years until the evolution of echocardiography. Operators have had so much experience with transesophageal echocardiography (TEE) that today transthoracic echocardiography (TTE) is a common procedure.
Although both short- and long-term follow-up results of percutaneous treatment are quite satisfactory, concerns have been raised regarding aortic erosion in the last few years.3) Since erosion may depend on device size, size calculations based on classically accepted balloon sizing are questioned. Instead of balloon sizing, many operators predict device size by adding constant numbers to the meticulously evaluated defect size using transesophageal echocardiography.4) This method may be most accurately used with three-dimensional (3D) transesophageal echocardiography which evaluates ASD dimensions most precisely. However, these constant numbers still rely on operator experience and not on scientific calculations. Although short-term results of this method seem successful, erosive complications should be followed up before the method suggested.
The atrial septum is an elastic structure which is permitted to distend. However, our experience suggests distensibility of the atrial septum differs between patients. Several factors may affect elastic tissue including age and genetic factors. In this study, we aimed to examine the relationship between age, sex, defect size, and atrial septum distensibility. We aim to guide operators when selecting devices depending on scientific criteria.
SUBJECTS AND METHODS
We retrospectively analyzed patients that underwent percutaneous ASD closure in our clinic at the Kartal Koşuyolu Heart Training and Research Hospital between January 2011 and December 2012. The study was approved by the local ethical committee. The study included patients whose ASDs were closed with Cardi-O-Fix (Starway Medical Technology, Inc., Beijing, China). Patients were included whose maximum defect size and device size were available. Finally, data for 66 patients were available and included in this study.
A two-dimensional (2D) TEE (Philips iE33; Philips Medical Systems, Andover, MA, USA) was used for pre-procedural evaluation. The procedure was performed with either TTE or TEE. When TTE was used, the patient was sedated. General anesthesia was used when the procedure was performed with TEE. Independent of defect and rim sizes, the balloon sizing technique was used in all procedures. Indentation on the slowly inflated balloon was measured under fluoroscopy. Thus, over-inflation of the balloon and overstretching of the defect were avoided. The same size device as the stretched defect size was used if available. A one size bigger device was used in instances when the same size was not available. Thus, a 2 mm bigger device than the stretched size could be implanted. The difference between device size and pre-procedural maximum defect size was accepted as the enlargement amount (EA). Hence enlargement ratio (ER) was acquired via dividing the EA by the pre-procedural maximum defect size. Calculations were formulated as follows:
Association of age, sex, and preprocedural maximum defect size with enlargement size and ratio were analyzed.
Statistical analyses
Statistical analyses were performed using SPSS 17.0 (SPSS Inc., Chicago, IL, USA). The Kolmogorov-Smirnov test was used to analyze data normality. Continuous data were expressed as mean±standard deviation (SD), and categorical data were expressed as percentages. The χ2 test was used to assess differences in categorical variables between groups. The relationships between parameters were assessed using Pearson's or Spearman's correlation analyses according to the normality of the data. Differences between patient subgroups were tested using the Mann-Whitney U or Student's t-tests where appropriate p value <0.050 was considered statistically significant.
RESULTS
A total of 66 patients, 19 (29%) male and 47 (71%) female aged 35.3±14.3 (min: 4, max: 65, median: 35.5) were included in this study. The study group included 4 children aged 4, 7, 13, and 15 years. The body mass index (BMI) for males and females was 25.5±5.5 and 25.1±4.2, respectively (p=0.850). Clinical presentations were as follows: 34 (51%) patients with dyspnea/fatigue, 12 (18%) patients with palpitation, 5 (7%) patients with chest pain, 1 patient with transient ischemic episode, 1 patient with cough, and 12 (18%) patients were asymptomatic. Only 1 patient had atrial fibrillation; the other 65 patients had sinus rhythm. Six patients had complete and 2 patients had incomplete right bundle branch block (RBBB) in electrocardiogram (ECG). Forty-seven (71%) patients had at least 1 of the echocardiographic findings of right atrial, right ventricular or pulmonary artery dilation and pulmonary artery pressure >36 mmHg. Forty (61%) procedures were performed with TEE and 26 (39%) with TTE. The success of percutaneous closure was 100%. Follow-up interval was 28±6 months. Residual shunt was detected in 2 (3%) patients and disappeared at follow-up. One patient had pericardial effusion which later disappeared. Early or late embolization did not occur.
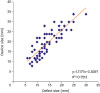
ASD size was 14.1±5.1 mm. Defect sizes for males and females were 13.7±4.4 mm (min: 7, max: 30, median: 14) and 15.7±6.4 mm (min: 6, max: 25, median: 13), respectively. ASD size was not different between the sexes (p=0.280). EA was 5.2±3.6 mm (min: 0, max: 15, median: 5) (Table 1). EA was not significantly different between the sexes (p=0.800). EA was not correlated with age or defect size (p=0.970; p=0.050). ER was 39.3%±31.5% (min: 0, max: 125, median: 32). Female and male ERs were 41.3%±32.3% and 34.5%±29.8%, respectively. ER did not differ between the sexes (p=0.430). ER was not significantly correlated with age and defect size (p=0.640; p=0.310). ER was less than 50% in 22 (88%) of 25 patients above 40 years of age (Figure 1). Patients were classified into younger and older groups with 40 as the cut-off. The ER of young and old patients was 46.8%±35.3% and 27.1%±18.8%, respectively, which was significantly different between the 2 groups (p=0.030). However, there were no differences between the 2 groups in terms of defect size and EA (p=0.120; p=0.110) (Table 2). The size of the deployed device was strongly correlated with defect size measured with 2D TEE (device size=1.1177×TEE defect size+3.5297; R=0.84; p<0.010) (Figure 2).
Table 1
Baseline characteristics

Values are presented as mean±SD or median (min, max).
BMI = body mass index; EA = enlargement amount; ER = enlargement ratio; SD = standard deviation.
![]()
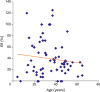
Table 2
ASD characteristics of young and older patients

| Characteristics | Age >40 (n=25) | Age ≤40 (n=41) | p value |
|---|---|---|---|
| Defect size (mm) | 15 (8, 25) | 13 (6, 30) | 0.120 |
| EA (mm) | 4 (0, 9) | 5 (0, 15) | 0.110 |
| ER (%) | 27.3 (0, 88) | 38.5 (0, 125) | 0.030 |
Values are presented as median (min, max).
ASD = atrial septal defect; EA = enlargement amount; ER = enlargement ratio.
![]()
DISCUSSION
We concluded that ER was lower in patients older than 40 years. Extracellur matrix regenenation ability tends to decrease with increased age which may result in loss of atrial septal elasticity. Probably atherosclerotic factors like diabetes, hypertension, dyslipidemia, and smoking could accompany a stiffened atrial septum. Since patients were rarely exposed to these degenerative factors before the 4th decade, we did not expect to see a linear relationship between ER and age.
Mean difference between deployed devices and maximal defect diameter was 5.2±3.6. Deployed devices were approximately 40% bigger than the defects. Although both EA and ER were widely dispersed, the ER in older patients was lower by approximately 27%. EA was not different between our groups despite the fact that defect sizes were similar. Mean values seemed to be similar to studies which used putative values to calculate device size without using balloon sizing.4) However, a wide range of values (min: 0, max: 15, median: 5) calculated in our study made it difficult to accept the mean value to decide device size. Despite this study restriction, it could be concluded that device size estimation without balloon dilatation would be feasible in older patients due to a stable ER (27%) and range (0–88).
Residual shunt and embolization ratios were compatible with other studies in the literature.5) This could be attributed to the precision of balloon sizing. Though higher ERs in patients younger than 40 can be explained by increased elasticity, doubt arising from overstretching is a factor which cannot be thoroughly eliminated. Although good correlation between device size and defect size is an indirect proof of precise balloon sizing, overstretching was strictly avoided. There may be another under-emphasized reason for over enlarging other than balloon over-dilatation. Non-circular ASDs were reported in up to 42% of different studies.6)7) Most of these defects are oval shaped rather than circle shaped which means these defects have 2 radii that are markedly different from each other. The balloon dilatation pattern of an oval shaped defect is evidently different from a circle shaped defect. A small radius tends to enlarge more compared with a large radius. Exact circular defects enlarge equally along both radii. Thus, circular defects enlarge more compared with oval defects. We lacked 3D data that could determine the impact of this intrinsic shape effect.
Defect sizes measured with 2D TEE are well correlated with devices and this can be mathematically formulated (device size=1.1177×TEE defect size+3.5297; R=0.84; p<0.010). Depending on this finding, it could be concluded that defect size is the most reliable measurement which guides device size estimation. Although the mathematical formula is strong, it is not possible to anticipate EAs and ERs when defects are observed one by one. Probably there are plenty of factors affecting enlargement parameters which make it impossible to include them all in a mathematical equation. The 3D structure of the defect could be much more important than any other factors. Despite these estimations and calculations, the experience of the operator in a particular technique still seems to be more decisive than other factors.
Although 4 decades have passed since the first percutaneous ASD closure and experience has increased tremendously, there is still debate about correct calculation of device size. The balloon sizing technique was accepted as the gold standard for determining device size since the first cases. The majority of operators still use balloon sizing and TEE conservatively. Du et al.8) observed 138 percutaneously closed defects and compared the differences between balloon sizing measurements and defects. They proposed the same size with an inflated balloon or a larger device up to 2 mm would be suitable for closure. In a study including 51 patients, Helgason et al.9) found significant discordance between defect sizes measured with 2D TEE and devices. Thus, they proposed that device deployment depending solely on defect size was not safe. In another study, ASDs of 41 patients were evaluated with 2D and 3D TEE and balloon sizing. The largest measurement was obtained with balloon dilatation, whereas the smallest was obtained with 2D TEE. 3D TEE measurements were so compatible with balloon sizing measurements that the study suggested 3D measurement could be used instead of balloon sizing. This study reported a similar correlation between 3D TEE and balloon sizing.10) However, that study emphasized 3D TEE would not be used as an alternative for balloon sizing, but rather could be used complementarily. Chien et al.11) compared balloon sizing measurements with intracardiac echocardiography (ICE), 2D TEE, TTE, and angiocardiography. Measurements with ICE correlated best with balloon sizing. Carlson et al.12) compared 2 different balloon sizing techniques. A compliant balloon was inflated until a significant waist appeared in 74 patients in the first group. The balloon was inflated till flow through the defect disappeared in 43 patients, but no waist appeared in the second group; later this technique was named, stop-flow. Five complications occured in the first technique, suggesting overstretching may not be as safe as thought before. Wang et al.4) conducted a study in order to clarify whether it was possible to precisely decide device size without balloon sizing. They compared 243 patients who underwent the procedure without balloon sizing and 271 patients with balloon sizing. In the group where balloon sizing was not used, the size of devices selected was 4–6 mm larger than the maximal diameter in case the defect was smaller than 14 mm and 5–8 mm larger in case the defect was equal to or larger than 14 mm. Closure and complication rates were similar between the 2 groups suggesting balloon inflation may not be necessary. Two embolizations occurred in each group, whereas no embolizations occurred in our study, though subject number was not sufficient to compare the studies. This finding may be attributed to the precision of balloon sizing in our study.
Two hundred thirty-four thousand atrial septal occluder (ASO) devices were used until 2011 since Food and Drug Administration (FDA) approval in 2002. The number of reported erosive complications was more than 100 with an incidence of approximately 0.1%–0.3%.13) The underlying etiology was not thoroughly clarified due to the rarity of complications. However, concerns raised about overstretching of the defect during balloon sizing resulting in larger device selection would be the underlying mechanism of erosion. Despite these concerns, the evidence is not enough sufficient to stop using balloon sizing. We perform balloon sizing rigorously so that we inflate the balloon slowly and do not inflate after a waist appears.
The retrospective nature of this study was a limitation for identifying balloon stretch diameters, thus more information is needed. We did not have a control group that was treated without balloon sizing. A paucity of child patients may also limit our ability to generalize this data.
In conclusion, we concluded that EA and ER were not associated with sex and defect size. However, ER was significantly larger in patients older than 40. Selected device size was correlated with maximal defect size measured on 2D TEE. Our results suggest it would be more appropriate to close ASDs without balloon sizing in older patients.
 XML Download
XML Download