

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Heart failure (HF) is an increasingly common cardiovascular syndrome and is the final pathway in several cardiac disorders.1) Many HF patients experience dyspnea, fatigue, diminished exercise capacity, and poor quality of life (QOL).
Progressive functional deterioration is common in HF patients because of exercise intolerance, but can be avoided by discouraging a sedentary lifestyle and promoting physical activity.2) Many recent randomized controlled trials have shown that exercise training (ET) programs enhance aerobic capacity, delay the onset of anaerobic metabolism, improve autonomic balance, decrease HF hospitalization, and increase survival.3)4)5) These trials comparing supervised hospital-based ET with educated home-based ET in HF patients lack data, especially among the Korean population. This study aims to compare the effects of both ET programs on the exercise capacity, QOL, and clinical outcomes of HF patients.
SUBJECTS AND METHODS
Patients
Patients were enrolled between September 2010 and February 2014 from referrals to the Cardiovascular Disease Prevention and Rehabilitation Center at Asan Medical Center, Seoul, Korea, which offers a multidisciplinary, outpatient cardiac rehabilitation program, providing supervised hospital-based ET, dietary and psychological counseling, and nursing education and support.
Symptomatic outpatients classified as New York Heart Association (NYHA) functional class I–III were selected. Included patients had at least 6 months of optimal and standard pharmacological treatment, left ventricular ejection fraction (LVEF) of 40% or less (according to the modified Simpson's method), and stable status for at least 3 months. Exclusion criteria were history of ventricular arrhythmia, implantation of a cardioverter-defibrillator or cardiac resynchronization therapy, pulmonary disease (vital capacity and/or forced expiratory volume in one second <80% of age-dependent predicted value), unstable angina, untreated coronary artery stenosis >50%, decompensated HF, hemodynamically significant valvular heart disease, uncontrolled hypertension (resting systolic blood pressure >150 mmHg or diastolic blood pressure >100 mmHg), anemia (hemoglobin <12 g/dL), clinically relevant musculoskeletal disease, clinically relevant arrhythmia, or change in cardiovascular medication within the previous four weeks. Of the 82 initial patients, 8 did not complete the ET program, 30 did not perform the follow-up cardiopulmonary exercise testing, and 44 completed the protocol (Figure 1).

The institution's Ethical Review Board approved this prospective study, and informed consent was obtained from each patient. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki, as reflected in a prior approval by the institution's human research committee.
Design
A non-randomized prospective trial compared a supervised hospital-based ET group with an educated home-based ET group. The study group was assigned according to the patient's decision. Patients underwent a physical examination, cardiopulmonary exercise testing, a 6-minute walk test, and blood sampling at baseline and after 3 months of ET. The Minnesota Living with Heart Failure Questionnaire (MLWHFQ) was used to assess QOL. Sonographers performed 2-dimensional echocardiographic examinations on all patients where LVEF was measured in the apical 4-chamber view and 2-chamber view using the modified Simpson's method.
Patients performed symptom-limited cardiopulmonary graded exercise testing on a COSMED Quark CPET metabolic cart (COSMED, Rome, Italy) with a Lode cycle ergometer (Lode Excalibur Sport; Lode B.V., Groningen, the Netherlands) beginning at a 20-watt workload and increasing by 15 to 25-watt increments every 2 minutes. Peak oxygen consumption (VO2) was measured directly breath-by-breath and defined as the average of 3 measurements recorded in the last minute of exercise. A 12-lead electrocardiogram was continuously recorded, blood pressure was measured every 2 minutes, and cardiopulmonary variables were calculated using printouts of 10-second averaged values. The hospital-based group participated in a structured, group-based exercise program with a goal length of 30–40 minutes, with one or 3 sessions each week for a total of 12 or 36 sessions in 3 months. Training intensity was tailored to 60% to 70% of the target heart rate reserve (maximum heart−resting heart rate).6) Exercises for the hospital group included treadmill walking, stationary cycling, arm ergometry, and stair climbing.
Patients in the home-based group participated in one session each month for 3 months with a formal exercise prescription. All patients received a detailed booklet of self-management educational materials at the time of enrollment, including information on medications, fluid management, symptom exacerbation, sodium intake, and moderate-intensity activity of 30 minutes (as tolerated) on most days of the week, consistent with guidelines from the American College of Cardiology and the American Heart Association.7)
Clinical outcomes
Follow-up started on the day the ET protocol began and ended with an adverse event. All patients were followed up every 2 months for at least one year after enrollment. The primary endpoint was a composite of all-cause mortality or hospitalization with worsening HF, defined as admission with new or increasing symptoms and signs of fluid retention, or objective evidence of HF and initiation of intravenous diuretic agents or vasoactive agents, mechanical ventilation, or mechanical support. All events were carefully verified and adjudicated by independent clinicians.
Statistical analysis
Data are expressed as mean±standard deviation (SD) for continuous variables and as frequency for categorical variables. Differences between groups were assessed using χ2 analysis for categorical variables and Student's t-test for continuous variables. Changes within the groups during follow-up were assessed by the t-test for paired variables. Survival curves for all-cause mortality or hospitalization with worsening HF were compared using Kaplan-Meier estimates and tested for statistical significance using the log-rank test at p<0.050. Event (or censoring) times for all patients were measured from the time of allocation (time zero). Statistical analysis was performed using commercially available software (SPSS 21 for Windows; SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline characteristics
Clinical characteristics of the 82 study patients according to ET type are presented in Table 1. There were no significant differences between the groups in terms of age, body mass index, NYHA functional classification, underlying diseases, medications, LVEF, or Dutch HF knowledge scales. The proportions of male sex and current smokers in the educated home-based group were higher than those in the supervised hospital-based group.
Table 1
Baseline characteristics of patients in the 2 treatment groups
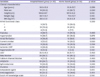
Values are presented as mean±SD or number (%).
ACEi = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; BMI = body mass index; CMP = cardiomyopathy; HF = heart failure; LVEF = left ventricular ejection fraction; NYHA = New York Heart Association; SD = standard deviation.
![]()
Exercise training effects
The changes from baseline in exercise time, peak VO2, 6-minute walk, and MLWHFQ scale at 3 months are presented in Tables 2 and 3. Significant improvements of exercise time and peak VO2 were observed in the supervised hospital-based ET group between the pre- and post-exercise periods. There were no such differences for the educated home-based ET group. The post-exercise differences between the 2 groups in exercise time and peak VO2 were statistically significant (p=0.010 for exercise time, p=0.014 for peak VO2). There was no significant difference between the pre- and post-exercise periods in the 6-minute walk for either group. Self-reported total MLWHFQ score improved significantly in the hospital-based group, but the difference between the groups was not statistically significant. There were no serious adverse events leading to early termination of ET such as ventricular arrhythmia, syncope, unstable angina, or worsening HF in any of the groups during the program.
Table 2
Comparison of the cardiopulmonary exercise test results and QOL between the pre- and post-exercise periods

Data are mean±SD or mean (95% CI). Complete case analysis. Expected 81 patients at 3 months.
CI = confidence interval; F/u = follow-up; MLWHFQ = Minnesota Living with Heart Failure Questionnaire; QOL = quality of life; SD = standard deviation; VO2 = oxygen consumption.
![]()
Table 3
Comparison of the cardiopulmonary exercise test results and QOL between the 2 groups

Data are mean (95% CI). Complete case analysis. Expected 81 patients at 3 months.
CI = confidence interval; MLWHFQ = Minnesota Living with Heart Failure Questionnaire; QOL = quality of life; VO2 = oxygen consumption.
![]()
Clinical outcomes
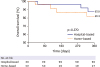
There were eight cardiac events during the one-year follow-up period, including 1 all-cause mortality in the supervised hospital-based ET group. Two patients in the hospital-based group and 5 patients in the home-based group were hospitalized with worsening HF (Table 4). The composite endpoint of all-cause mortality or hospitalization with worsening HF was not statistically different in the 2 groups (Figure 2; hazard ratio [HR], 0.66; 95% confidence interval [CI], 0.2–2.8; p=0.570). We analyzed the post-exercise clinical outcome according to the number of exercise sessions. However, event-free survival did not correlate with number of exercise sessions (Figure 3).
Table 4
Clinical outcomes in the 2 groups

CI = confidence interval; HF = heart failure; HR = hazard ratio.
*HR of the hospital-based group compared to the home-based group.
![]()

DISCUSSION
Significant improvement in functional capacity, exercise capacity, and QOL was observed in the supervised hospital-based group following the 12-week cardiac rehabilitation program. The composite endpoint of all-cause mortality or hospitalization with worsening HF was not different between the groups for one year after cessation of the ET program.
HF is a common clinical syndrome caused by a variety of cardiac diseases. After an initial reduction in cardiac output, intrinsic cardiac decline leads to systemic deterioration with a reduced ability to exercise, early fatigue, weakness, and shortness of breath.8) Such symptoms impact the performance of activities of daily living and significantly contribute to reduced participation and poor QOL.9)
ET is a valuable adjunct in the therapeutic approach to stabilize HF patients and is a class I recommendation from the American College of Cardiology and the American Heart Association.10) Most studies of exercise in HF patients have focused on hospital-based programs where patients exercise under controlled conditions. Many Korean HF patients are unable to access a formal ET program because they live in remote geographic locations, have difficulty with transportation, or do not have the financial resources to pay for a structured ET program. Furthermore, HF patients with functional limitations demonstrated poor cognitive function and self-care confidence, which can interrupt active participation in a hospital-based ET program.11) Since a home-based program is optimal for these patients, the comparison between hospital- and home-based ET programs has great clinical implications.
Peak VO2 improved in the hospital-based group by 2.5 mL/min/kg compared to the home-based group (95% CI, 0.5–4.4; p=0.014) at cessation of the ET program, along with an improved exercise time of 65.2 seconds (95% CI, 14.0–116.5; p=0.010). This is an encouraging result, as the improvement and sustainability of functional performance are the primary goals of an ET program. Exercise capacity increase was modest in the hospital-based ET group, with an improvement rate in measured peak VO2 of about 10%, relatively lower than in other studies.12)13) There was no improvement in the home-based ET group. Considering the numerical improvement of QOL in both groups, modest or no improvement in exercise capacity might result from the poor clinical conditions or comorbidities of patients rather than inadequate exercise.
Among the exercise parameters, the 6-minute walk was not significantly improved in either group (21.9 vs. 2.0 m, p=0.330). The 6-minute walk offers a convenient and economical clinical test of functional performance compared with normal activity,14) but has several limitations. The test provides no insight into the mechanisms of exercise limitation, and its results can be affected by unrelated factors such as age, sex, height, and weight. The benefits of ET should therefore not be underestimated, irrespective of the program type.
A number of studies have found an increase in QOL with ET.15)16) Some studies have demonstrated improved QOL with little or no change in exercise capacity.17)18) This study found a significant improvement of QOL in the supervised hospital-based ET group and numeric improvement of QOL in the educated home-based ET group. These findings suggest that QOL improvement can occur even with modest or no change in exercise capacity. It is further suggested that QOL is determined not only by physiologic change, but also by factors affecting the patient's perception of health.
ET improves cardiac output and regional blood flow, which are associated with increased peak VO2. HF patients with a higher peak VO2 have a greater survival rate. Therefore, improving peak VO2 can improve survival and reduce hospitalization. Alterations in the autonomic nervous system that decrease sympathetic tone and increase vagal tone might have similar effects.19) Hospital-based ET did not provide a significant reduction in the composite endpoint of all-cause mortality or hospitalization with worsening HF, which was not in concordance with other studies.3)5) The home-based ET group in this study differed from groups in other studies, as patients were educated with a formal exercise prescription one or 3 times for effective ET at home. These patients might have increased exercise intensity or duration because of the unblinded assignment, possibly affecting the results between the program types in clinical outcomes over 1 year.
This study has several limitations. It was a non-randomized trial where patients who agreed to and were available for participation could be systematically different from those unable to participate, which could limit the generalizability of the findings. The 82-patient population was relatively small and was derived from a single center, and patients were young compared to the general population with HF. Thirty-eight (20% of the hospital-based group; 62% of the home-based group) of the total study patients terminated the ET program prematurely or did not perform the follow-up functional test because of health insurance issues. However, clinical follow-up was performed every 2 months in the HF outpatient clinic, assessing the occurrence of clinical events in all patients. Clinical outcomes of the non-follow-up patients were not different compared to those of the follow-up patients (Supplementary Figure 1). Finally, adherence to the ET was not assessed because it was difficult to objectively evaluate whether or not practicing ET at home made a difference. This is a major limitation of our study and could be a bias that affected the results.
In conclusion, the present study demonstrated that supervised hospital-based ET was beneficial for HF patients with improving functional capacity and QOL. However, hospital-based ET provided a non-significant reduction in the risk for the composite endpoint of all-cause mortality or hospitalization of worsening HF compared to the home-based ET program. In cases that were unsuitable for supervised hospital-based ET, educated home-based ET with a detailed exercise prescription could be considered as an alternative option for the non-pharmacological treatment for HF. Further well-designed large studies are needed to define the role and effect of hospital-based or home-based ET programs.
 XML Download
XML Download