

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Heart failure (HF) is the leading cause of death and hospital admission in the United States and worldwide including Korea. Its incidence and prevalence are increasing, and it has a substantial mortality and morbidity rate.1)2)3)
There exist bidirectional interactions between heart and kidney, and clinical conditions in which either the diseased kidney or heart makes the other organ dysfunctional; this is defined as cardio-renal syndrome (CRS). The proposed mechanisms include neurohormonal (i.e., autonomous nerve system, renin-angiotensin-aldosterone system, and natriuretic peptide system), and hemodynamic factors (i.e., arterial pressure and venous congestion).4)
N-terminal pro-brain natriuretic peptide (NT-proBNP) is a biomarker used to evaluate the degree of neurohormonal activation.5)6) Patients with HF with reduced ejection fraction (HFrEF) have higher NT-proBNP levels than those with preserved ejection fraction (HFpEF) suggesting they have different degrees of neurohormonal activation.7)8) Considering that NT-proBNP reflects the level of neurohormonal activation and patients with HFrEF had higher levels of NT-proBNP, the prevalence and prognostic value of renal dysfunction may be dependent on the type of HF.
In this study, we first investigated the relationship of renal function with left ventricular (LV) systolic function, and NT-proBNP level. Second, we examined the prevalence and prognostic value of renal dysfunction in HFpEF vs. HFrEF.
MATERIALS AND METHODS
Patients and data collection
The Korean Heart Failure (KorHF) Registry is a prospective multicenter registry designed to reflect the real-world clinical data of Korean patients admitted for acute heart failure (AHF). The study design and the primary results of the KorHF registry have been published elsewhere.9)
The registry was founded in June 2004 and is supported by the Korean Society of Heart Failure. Twenty-four well-qualified centers participated in the registry. All consecutive patients hospitalized with an episode of AHF as the primary reason for admission were eligible for enrolment. HF was diagnosed at admission according to the Framingham criteria.10)
Patients with new-onset (de novo) AHF as well as those with acutely decompensated HF (ADHF) were included. ADHF was defined as worsening of HF in patients with a previous diagnosis or hospitalization for HF. New-onset AHF was defined as AHF in patients with no previous history of HF. A confirmed diagnosis of HF at discharge was also required. All patients were strongly recommended for follow-up assessments for at least 1 year, and follow-up outcome data including mortality and re-hospitalization because of HF, were prospectively collected using medical records and by telephone contact. The mean observational period was 1.7 years (range, 0.1–4.9 years), from June 2004 to April 2009. The institutional review board or ethics committee at each participating hospital approved the study protocol and patients gave written informed consent before study entry. The investigation conformed to the principles outlined in the Declaration of Helsinki.
For laboratory tests, leukocytes, hemoglobin, blood urea nitrogen (BUN), creatinine (Cr), serum sodium, troponin I, and NT-proBNP levels measured at admission were collected for the registry. Blood sampling and tests were conducted as routine practice by laboratories at each center certified by The Korean Association of Quality Assurance for Clinical Laboratory. Patients underwent echocardiographs during hospitalization for AHF. Estimated glomerular filtration rate (eGFR) was calculated from Cr values using the modification of diet in renal disease (MDRD) formula.11) Preserved renal function and renal dysfunction were defined as GFR≥60 mL/min/1.73 m2 and GFR<60 mL/min/1.73 m2, respectively. Patients with renal dysfunction were further classified as mild (30≤GFR<60 mL/min/1.73 m2) and severe renal dysfunction (<30 mL/min/1.73 m2). HFpEF and HFrEF were defined as left ventricular ejection fraction (LVEF) ≥50% and LVEF<50%, respectively.12)13) Data were collected at each site by a trained study coordinator using a standardized case report form and entered into the KorHF Registry database via a web-based electronic data capture system that included an electronic case report form. Data collection and audition were performed by the KorHF Registry Steering Committee at the Korean Society of Heart Failure.
Endpoints
The primary endpoint was 12-month all-cause death stratified by renal dysfunction and LVEF.
Statistical analysis
Data were presented as numbers and frequencies for categorical variables, and as mean±standard deviation (SD) or median with interquartile ranges for continuous variables. For comparison between groups, the χ2 test (or Fisher's exact test when any expected cell count was <5 for a 2×2 table) was used for categorical variables and unpaired Student's t-tests were applied for continuous variables. We calculated the area under the curve (AUC) of LVEF and log NT-proBNP level by receiver-operating-characteristics analysis to predict renal dysfunction. Kaplan-Meier curves were plotted and compared with the log-rank test. A multivariate Cox proportional hazards regression model was used to identify the independent predictors of all-cause death. Variables either associated with mortality with p<0.050 or reported to be associated with mortality were included as confounding variables in the multivariate analysis: age, sex, previous history of myocardial infarction, congestive HF, peripheral artery disease, chronic lung disease, diastolic blood pressure, hemoglobin, serum sodium, GFR, and NT-proBNP. Two-sided p values <0.050 were considered statistically significant. Statistical tests were performed using IBM SPSS Statistics version 22 (SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline characteristics of the study population
Three-thousand two-hundred consecutive hospitalized AHF patients were enrolled in the KorHF Registry. Mean age was 67.6 years old and 50% were male, 47% had hypertension and 31% had diabetes mellitus (DM). The overall 1-year mortality rate was 15%. Among them, GFR, LVEF, and NT-proBNP levels were available for 1,932 patients (60%). Mean age was 68 years and 49% were male. Of these, 47% had hypertension, and 30% had DM, and 78% were New York Heart Association (NYHA) functional class III or IV. The mean ejection fraction (EF) was 39% and that of GFR was 62 mL/min/1.73 m2.
Overall, 51% had renal dysfunction; among them 38% had mild and 14% had severe renal dysfunction. Patients with renal dysfunction had more unfavorable baseline characteristics (Supplementary Table 1). With regard to LV systolic function, 524 patients (27%) were diagnosed with HFpEF and they had more unfavorable baseline characteristics, such as older age and higher prevalence of hypertension (Supplementary Table 2). The baseline characteristics of the patients according to renal dysfunction and EF are shown in Table 1. Patients with renal dysfunction were older. In addition, they had higher prevalence of DM, hypertension, myocardial infarction, and stroke history in both HFpEF and HFrEF groups. Concerning the laboratory parameters, patients with renal dysfunction showed lower hemoglobin, serum sodium level, and higher NT-proBNP level regardless of HFpEF and HFrEF.
Table 1
Baseline characteristics according to GFR and LV systolic function

BUN = blood urea nitrogen; Cr = creatinine; DM = diabetes mellitus; EF = ejection fraction; GFR = glomerular filtration rate; HF = heart failure; HFpEF = heart failure with preserved ejection fraction; HFrEF = heart failure with reduced ejection fraction; LV = left ventricle; NT-proBNP = N-terminal pro-brain natriuretic peptide; NYHA = New York Heart Association; SD = standard deviation.
The relationship between log NT-proBNP, EF, and GFR
There was a significant inverse correlation between GFR and log NT-proBNP level in all (r=−0.298, p<0.001), HFpEF (r=−0.359, p<0.001), and HFrEF patients (r=−0.284, p<0.001). Consequently, patients with renal dysfunction had higher log NT-proBNP levels than their counterparts (3.47 [3.09–3.79] vs. 3.85 [3.48–4.24]; p<0.001). Furthermore, there was an inverse correlation between LVEF and log NT-proBNP levels (r=−0.238, p<0.001), so that HFrEF patients had higher log NT-proBNP levels than HFpEF patients (3.02 [3.44–3.78] vs. 3.74 [3.37–4.07]; p<0.001]. GFR did not correlate with LVEF (r=0.017, p=0.458), and there was no difference in GFR between the HFpEF and HFrEF (62.8±34.1 vs. 61.3±40.5 mL/min/1.73 m2; p=0.462). Consequently, there was no difference in the prevalence of renal dysfunction between the 2 groups, either (49% vs. 52%; p=0.210) (Supplementary Figure 1A-F). There was no significant difference in NT-proBNP level whether patients were diagnosed as de novo HF or ADHF (median, 4,377.0 vs. 4,941.0; p=0.168).
In receiver-operating-curves analysis, the AUC of log NT-proBNP level to predict renal dysfunction was 0.71 (95% confidence interval [CI], 0.69–0.73) in all patients, 0.71 (95% CI, 0.66–0.75) in HFpEF and 0.71 (95% CI, 0.69–0.74) in HFrEF patients. In contrast, the AUC of EF was only 0.51 (95% CI, 0.48–0.53) in all patients, 0.52 (95% CI, 0.47–0.57) in HFpEF and 0.54 (95% CI, 0.51–0.57) in HFrEF patients (Figure 1). The risk of renal dysfunction increased with NT-proBNP levels, but not with LVEF (Figure 2).
Figure 1
Association between renal dysfunction according to log NT-proBNP and LVEF. In receiver-operating-curves analysis, the AUC of log NT-proBNP (A) and LVEF (B) to predict renal dysfunction are presented.
AUC = area under the curve; CI = confidence interval; EF = ejection fraction; HFpEF = heart failure with preserved ejection fraction; HFrEF = heart failure reduced ejection fraction; LVEF = left ventricular ejection fraction; NT-proBNP = N-terminal pro-brain natriuretic peptide.

Figure 2
Association of NT-proBNP and LVEF with renal dysfunction.
Patients were divided in quartiles according to LVEF and NT-proBNP. Risk on the y-axis is HR±95% CIs using a logistic regression model.
CI = confidence interval; HR = hazard ratio; LVEF = left ventricular ejection fraction; NT-proBNP = N-terminal pro-brain natriuretic peptide; OR = odds ratio.

Independent predictors of renal dysfunction were old age (odds ratio [OR], 1.50; 95% CI, 1.18–1.90), being female (OR, 1.40; 95% CI, 1.12–1.75), having DM (OR, 1.63; 95% CI, 1.28–2.07), hypertension (OR, 1.99; 95% CI, 1.59–2.48), history of congestive HF (OR, 1.59; 95% CI, 1.25–2.03), myocardial infarction (OR, 1.75; 95% CI, 1.26–2.43), hemoglobin<11.5 mg/dL (OR, 1.91; 95% CI, 1.52–2.39), serum sodium<135 mmol/L (OR, 1.61; 95% CI, 1.22–2.14), and log NT-proBNP ≥3.65 pg/mL (OR, 2.70; 95% CI, 2.18–3.35).
Clinical outcomes according to EF and renal dysfunction
At 12-month follow-up, 241 patients (12.5%) died and 372 patients (19.3%) were readmitted. Patients who died had more unfavorable baseline characteristics, such as older age, previous history of myocardial infarction, congestive HF, peripheral artery disease and chronic lung disease. They had lower levels of hemoglobin, but higher levels of BUN, serum Cr, and NT-proBNP (Supplementary Table 3).
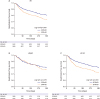
Patients with renal dysfunction had higher 12-month mortality (8.4% vs. 16.4%; log-rank p<0.001). When stratifying according to HF type, patients with renal dysfunction had higher mortality in both HFpEF (7.9% vs. 15.2%; log-rank p=0.008) and HFrEF (8.6% vs. 16.8%; log-rank p<0.001) groups (Figure 3). Survival analysis of 4 groups according to LVEF and renal dysfunction is presented in Supplementary Figure 2. Concerning readmission, patients with renal dysfunction had a higher readmission rate (16.5% vs. 21.9%; log-rank p<0.001), however, when stratifying according to EF, patients with renal dysfunction had higher readmission only in the HFrEF (16.6% vs. 23.3%; log-rank p<0.001), but not in the HFpEF group (16.1% vs.18.0%; log-rank p=0.479) (Figure 4). With regard to severity of renal dysfunction, patients with severe renal dysfunction had worse outcomes (Supplementary Figures 3 and 4).
Figure 3
Survival rates according to renal dysfunction. Kaplan-Meier curves of the 12-month survival rates according to renal dysfunction in all (A), HFpEF (B), and HFrEF (C) patients are presented.
GFR = glomerular filtration rate; HFpEF = heart failure with preserved ejection fraction; HFrEF = heart failure with reduced ejection fraction.
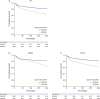
Figure 4
Readmission free survival rates according to renal dysfunction. Kaplan-Meier curves for 12-month readmission free survival rates according to renal dysfunction in all (A), HFpEF (B), and HFrEF (C) patients are presented.
GFR = glomerular filtration rate; HFpEF = heart failure with preserved ejection fraction; HFrEF = heart failure with reduced ejection fraction.
In a Cox proportional hazard regression analysis, renal dysfunction was a significant predictor of 12-month mortality (mild renal dysfunction and hazard ratio [HR], 1.33; 95% CI, 0.65–2.70; severe renal dysfunction and HR, 2.08; 95% CI, 1.40–3.11) amongst others (Table 2). When stratifying according to HF type, severe renal dysfunction was a significant risk factor in HFrEF patients (HR, 2.43; 95% CI, 1.52–3.89). But its prognostic value was diminished in HFpEF patients (HR, 1.46; 95% CI, 0.66–3.21 across 30 mL/min/1.73 m2).
Table 2
Multivariate Cox regression analysis for all-cause mortality

CI = confidence interval; GFR = glomerular filtration rate; HF = heart failure; HFpEF = heart failure with preserved ejection fraction; HFrEF = heart failure with reduced ejection fraction; HR = hazard ratio; NT-proBNP = N-terminal pro-brain natriuretic peptide.
*HRs have been adjusted for age >65 years, sex, previous history of myocardial infarction, congestive HF, peripheral artery disease, chronic lung disease, diastolic blood pressure < median, hemoglobin < median, and serum sodium level <135 mmol/L.
DISCUSSION
The main findings of this multicenter HF registry analysis are as follows; GFR was dependent on log NT-proBNP level, but independent of EF; and the prevalence of renal dysfunction was similar in HFpEF and HFrEF groups. Renal dysfunction was an independent risk factor for poor outcomes in all AHF patients. However, its prognostic value was attenuated in HFpEF patients, suggesting a differential prognostic value according to HF type.
It is of note that there was a significant inverse correlation between log NT-proBNP level, GFR, and LVEF; however, there was no significant correlation between GFR and LVEF, and the proportion of renal dysfunction was the same in HFpEF vs. HFrEF. The inverse relationship between log NT-proBNP levels and renal function has been previously reported.14)15) Although the renal dependence on clearance of NT-proBNP partly accounts for elevation of NT-proBNP level, the wide variation in NT-proBNP level among patients with renal dysfunction suggests that reduced renal clearance is only one of many mechanisms for NT-proBNP elevation.14) NT-proBNP is a cardiac neurohormone that is mainly secreted from the ventricles in response to an increase in wall tension.16) According to the law of Laplace, wall tension correlates directly with wall pressure and LV diameter, but inversely with LV wall thickness. Thus, HFrEF patients with an enlarged LV cavity size have higher wall tension and higher NT-proBNP levels than HFpEF patients with an increased relative wall thickness and relatively preserved LV diameter.17)
Renal dysfunction in HF patients comprises 2 main components; i.e., intrinsic nephropathy and CRS. As for the intrinsic nephropathy, both HF and kidney disease share common comorbidities such as old age, hypertension, and DM. Nonetheless, these risk factors were more prevalent in HFpEF, so that we cautiously speculate that the proportion of intrinsic nephropathy may be higher in HFpEF than in HFrEF patients. Various comorbidities including DM are reported to cause endothelial inflammation in the microvasculature, leading to functional and structural abnormalities contributing to HFpEF development.18)19) Those comorbidities can also cause renal impairment by microvascular dysfunction, implying that HFpEF patients may at higher risk for renal impairment.20)21)
Concerning CRS, impaired hemodynamic status and excessive neurohormonal activation are the most often discussed mechanisms. In HF patients, inadequate renal perfusion due to low cardiac output, renal venous congestion, and excessive vasoconstriction can cause impaired renal function. Tang and Mullens22) showed in AHF patients with low LVEF, venous congestion was the strongest hemodynamic determinant for the development of worsening renal function, while impaired cardiac index had a limited contribution.12) This explains the lack of correlation between GFR and LVEF, because LVEF does not necessarily translate into cardiac index. NT-proBNP is a biomarker for neurohormonal activation and HFrEF patients had higher NT-proBNP levels. We also cautiously suggest that the proportion of CRS patients may be higher in HFrEF than in HFpEF.
Taken together, the different proportion of intrinsic nephropathy and CRS may explain the phenomenon of same prevalence of renal dysfunction in HFpEF and HFrEF despite the difference in NT-proBNP levels. In the candesartan in heart failure: assessment of reduction in mortality and morbidity (CHARM)-overall program, there was no correlation between GFR and LVEF, and patient proportion with renal dysfunction was 34.7% in the CHARM-preserved, 33.0% in CHARM-added, and 42.6% in CHARM-alternative study, respectively.23) This may also explain the differential prognostic impact of impaired renal function on outcomes by LVEF.
Renal dysfunction is a well-known risk factor for worse clinical outcomes in HF patients.12)24)25) In this study we also showed that HF patients with renal dysfunction had higher 12-month mortality and readmission rates compared to those without renal dysfunction. However, when stratifying according to the EF, the prognostic value of renal dysfunction differed; in the HFrEF group, severe renal dysfunction was associated with an increased risk of 12-month mortality, while in the HFpEF group, its prognostic value was not statistically significant after adjustment for significant covariates.
The impact of renal function on survival has been well studied in HFrEF patients, and patients with renal dysfunction showed poor prognosis.25)26)27) However, in patients with HFpEF, the data are limited. Rusinaru et al.28) showed that HFpEF patients with impaired function (defined as GFR<60 mL/min/1.73 m2) had a 1.43 fold increased risk for 7-year mortality, but no increase at 6 months. In the CHARM study, renal dysfunction had poor prognosis for both HFrEF and HFpEF patients.23) In a post-hoc propensity score analysis of the digoxin investigation group (DIG) trial, the chronic kidney disease (CKD)-associated mortality was worse in patients with diastolic HF than in those with systolic HF.29) The reason for the different prognostic impact between studies including ours may be explained by the different study populations, definitions of HFpEF, and study periods (Supplementary Table 4).
In our study, the 1-year survival did not differ between HFpEF and HFrEF patients (log-rank p=0.527, Supplementary Figure 5), which is in line with previous studies.12) Our results suggest that the contribution of renal dysfunction to worse outcomes seems to be attenuated in HFpEF. The HFpEF patients had more unfavorable baseline characteristics such as older age and hypertension among others; it is possible that the effect of renal dysfunction on outcomes may be diluted by other risk factors.
It is of note that NT-proBNP level remained a strong prognostic factor in both HFpEF and HFrEF patients.8) Thus, NT-proBNP seems to be a more robust prognostic marker for clinical outcomes than renal impairment, regardless of the type of HF.
Our study has several limitations. First, this is an analysis of a prospective cohort, albeit a large one, rather than a randomized trial, and therefore unmeasured confounding factors could have an influence on the relation between renal insufficiency, LV systolic function and clinical outcomes. Second, we only included patients who had available data on EF, NT-proBNP level and GFR. Thus, we cannot exclude the possibility of selection bias. Third, we used the MDRD formula to calculate GFR which should be used for patients with stable renal function. The accuracy of the MDRD formula may not be warranted in AHF patients. Because we used LVEF during admission for AHF to classify HF, we do not know how many patients would be reclassified to chronic stable HF status, when considering the wide variation of LVEF between acute and chronic HF. Nonetheless, categorization during the acute phase has been widely accepted.9)17) Finally, pulmonary function tests were not routinely performed in these patients. Although there was no significant difference in previous history of chronic lung disease between HFpEF and HFrEF groups in this registry, this could introduce misdiagnosis of chronic obstructive lung disease to HFpEF.30)
In conclusion, in AHF patients, the prevalence of renal dysfunction did not differ between HFpEF and HFrEF patients. Renal dysfunction was independent of LV systolic function, but dependent on NT-proBNP level. Although severe renal dysfunction is a significant prognostic factor in HFrEF patients, its impact seems to be attenuated in HFpEF patients.
 XML Download
XML Download