

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Ticagrelor is considered a more potent antiplatelet agent than clopidogrel and is often used in patients with acute coronary syndrome (ACS). Ticagrelor demonstrated significant reduction in the composite incidence of death, myocardial infarction (MI), or stroke without concomitant increases in major bleeding in the Platelet Inhibition and Patient Outcomes (PLATO) trial, a multicenter, randomized study comparing ticagrelor with clopidogrel across a broad spectrum of ACS patients.1) Although the mechanism of action resulting in superior outcome with ticagrelor is not clear, several mechanisms have been suggested.
In addition to potent inhibition of platelets, ticagrelor increased adenosine plasma concentration in patients with non-ST-elevation ACS compared to clopidogrel by inhibiting adenosine reuptake by erythrocytes.2) Extracellular adenosine has a wide spectrum of positive physiological effects including vasodilation, release of endothelial factors, and cardioprotective and anti-inflammatory effects. Moreover, some animal studies demonstrated that ticagrelor reduced myocardial infarct size via adenosine-receptor activation.3)4) However, there is limited data in humans, especially in patients undergoing primary percutaneous coronary intervention (PCI).
We designed a prospective study to compare the effects of ticagrelor and clopidogrel on myocardial infarct size assessed by technetium-99m (Tc-99m) tetrofosmin single-photon emission computed tomography (SPECT) in patients with ST-segment elevation myocardial infarction (STEMI) undergoing primary PCI.
SUBJECTS AND METHODS
Study population
The present study employed a single-center, randomized, open-label design to compare the effect of ticagrelor loading dose with clopidogrel loading dose. From February 2014 to June 2016, consecutive patients who underwent primary PCI for STEMI were enrolled. Patients who were at least 20 years of age and who were within 24 hours of STEMI symptom onset with documented ischemia due to significant lesion in a native coronary artery were recruited. Exclusion criteria were patients more than 80 years of age, cardiogenic shock, oral anticoagulation therapy, previous history of intracranial bleeding, and previous medication with P2Y12 receptor blocker.
Risk factors such as previous history of hypertension or current antihypertensive therapy, diabetes treated with insulin or oral antihyperglycemic agent, baseline HbA1c >6.5%, and any type of smoking in the last month were recorded. All patients provided informed consent for processing their anonymous data according to a protocol approved by the Institutional Review Board of Wonkwang University Hospital.
PCI
In all patients, aspirin (300 mg/day) was loaded before the procedure. An intravenous bolus of 5,000 U of unfractionated heparin was given, and then additional heparin boluses were given to maintain activated clotting time >300 seconds during the procedure. Coronary angiography and stent implantation were performed using standard interventional techniques. Platelet glycoprotein IIb/IIIa inhibitors (GPIs) were administered according to operator decision. Aspirin (100 mg/day), clopidogrel (75 mg/day), or ticagrelor (180 mg/day) and statins were prescribed to all patients after the procedure.
Myocardial infarct size and angiography analyses
Pre- and post-PCI angiograms were reviewed. The thrombolysis in myocardial infarction (TIMI) flow grade before and after PCI, corrected TIMI frame count (cTFC), and myocardial blush grade (MBG) were analyzed by 2 experienced observers who were blinded to patient groups, as described previously.5)6)
Myocardial infarct size was measured by SPECT imaging and enzymatic methods. Creatine kinase-myocardial band (CK-MB) isoenzyme and troponin T were measured before and at 8, 24, and 48 hours after primary PCI. Peak concentrations were identified, and the area under time-concentration curves was estimated from cardiac biomarker levels measured at individual time-points.
SPECT imaging with Tc-99m tetrofosmin was performed by a standardized technique. After injection of adenosine, 370 MBq of Tc-99m tetrofosmin was intravenously injected, and stress myocardial images were obtained. After 4 hours, another 1,110 MBq of Tc-99m tetrofosmin was intravenously administered, and resting myocardial images were obtained. The SPECT images were acquired on a dual-headed gamma camera (Vertex 60, Philips ADAC, Milpitas, CA, USA) equipped with high-resolution collimators. Myocardial perfusion defects (infarct size) were quantified and expressed as percentage of involved left ventricle by a specialist who was unaware of the patient groups. Patients underwent SPECT imaging for a median of 2 days (interquartile range [IQR], 2–3 days) after PCI.
Study endpoints
The primary endpoint was myocardial infarct size, as assessed by SPECT. Secondary endpoints included 1) TIMI flow grade, cTFC, MBG after PCI; and 2) infarct size assessed by serial cardiac biomarker measurement.
Statistical analysis
Based on previous data from Wonkwang Medical Center, the infarct size of the control group was expected to be 20% (standard deviation [SD] 15%).7) The sample size was selected to demonstrate reduced infarct size from 20% in the clopidogrel group to 14% in the ticagrelor group (30% relative reduction) based on a previous statin study.7)8) A minimal sample size of 85 patients in each group provided 85% power with a 2-sided alpha of 0.05.
All measurements were represented as mean±SD or absolute number (percentage). Inter-group analysis was performed using independent t-test and χ2 test, which were conducted using Statistical Package for the Social Sciences (SPSS) version 19.0 for Windows (SPSS Inc., Chicago, IL, USA). To compare changes in cardiac biomarkers before and after PCI, paired t-test was used. Statistical significance was set at p<0.050.
RESULTS
Baseline characteristics
A total of 194 patients were eligible; of these, 97 patients received 300 mg clopidogrel as a loading dose (clopidogrel group), and 97 patients received 180 mg of ticagrelor as a loading dose before primary PCI (ticagrelor group). Two patients died before undergoing SPECT imaging, 2 patients were excluded due to absence of a significant coronary lesion, 1 patient was excluded for refusal to undergo SPECT, and 1 patient was excluded because of inadequate imaging. Therefore, 92 patients in the clopidogrel group and 96 patients in the ticagrelor group were finally evaluated for myocardial infarct size (Figure 1).
Figure 1
Study flow chart.
ICH = intracranial hemorrhage; MI = myocardial infarction; PCI = percutaneous coronary intervention; SPECT = single-photon emission computed tomography; STEMI = ST-segment elevation myocardial infarction.

The baseline clinical characteristics of patients in both groups are shown in Table 1. The clopidogrel group had a higher incidence of diabetes (30.4% vs. 14.6%; p=0.014) than the ticagrelor group, and the ticagrelor group had a higher level of low-density lipoprotein (LDL) cholesterol (104.6±40.8 mg/dL vs. 118.0±44.3 mg/dL; p=0.036) than the clopidogrel group. Other risk factors, including door-to-balloon time and baseline cardiac biomarker levels, were similar between the groups. All patients received second-generation drug-eluting stents (Table 2). Most angiographic and procedural characteristics were similar between groups, but patients in the clopidogrel group received more GPI than those in the ticagrelor group (23.9% vs. 9.4%; p=0.007).
Table 1
Baseline clinical characteristics

Table 2
Coronary angiographic and procedural characteristics
Primary endpoint
Median infarct size assessed by SPECT was 21.0% (IQR, 8.0%–41.0%). There was no difference in the time from PCI to SPECT between the groups (Table 3). Mean myocardial infarct size was similar between the 2 groups (28.1%±34.5% vs. 32.8%±29.2%; p=0.169). In subgroup analyses, there were no differences in infarct size with respect to age, gender, presence of diabetes, anterior MI, use of glycoprotein inhibitor, onset-to-door time, and stent length (Table 4).
Table 3
Radionuclide imaging and angiographic outcomes

Table 4
Comparison of infarct size (%) in specific risk subgroups

Secondary endpoint
Angiographic no reflow and final TIMI flow grade <3 occurred at a similar rate in both groups (Table 3). Final cTFC and MBG were also similar between the 2 groups.
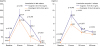
At all time-points after PCI (8, 24, and 48 hours), peak levels of CK-MB and troponin T were lower in the clopidogrel group (Figure 2). The clopidogrel group showed lower cumulative troponin T levels (12.59±10.66 vs. 17.67±19.51 ng/mL; p=0.029) compared to the ticagrelor group.
DISCUSSION
In this study, we fail to demonstrate that ticagrelor loading before primary PCI reduces myocardial infarct size compared to clopidogrel loading. Despite the beneficial effects of ticagrelor in previous experimental studies,3)4) ticagrelor did not improve infarct size in patients with STEMI, as assessed by SPECT and cardiac biomarkers.
Ticagrelor is a potent P2Y12 antagonist and has clinically proven beneficial effects in patients with ACS.1) Its beneficial mechanism is explained by platelet inhibition and extra-platelet effects. Ticagrelor increases plasma adenosine concentration. The maintenance dose of ticagrelor was reported to augment adenosine-induced coronary blood flow velocity in non-ST-elevation ACS patients undergoing PCI.9) Similar to maintenance dose, a single 180 mg loading dose of ticagrelor enhanced adenosine-induced coronary blood flow velocity in a double-blind, randomized study including 40 healthy male subjects.10)
Ticagrelor might be able to stabilize plaque. Lee et al.11) first reported the presence of P2Y12 receptor in human coronary atherosclerotic plaque. Apart from their antiplatelet actions, it is likely that P2Y12 antagonists might also have anti-ischemic effects secondary to induced plaque stabilization. Ticagrelor, due to its pharmacokinetic superiority over clopidogrel, is probably more powerful in this regard.
Ticagrelor might also have a cardioprotective effect. One animal study demonstrated that ticagrelor significantly reduced infarct size assessed by cardiac magnetic resonance imaging (MRI) compared to clopidogrel.4) Ticagrelor was demonstrated to reduce necrotic injury and edema resulting from an adenosine-dependent mechanism. In patients with STEMI, Park et al.12) reported that ticagrelor improved microvascular injury assessed by an index of microcirculatory resistance and reduced infarct size assessed by cardiac biomarker assay.
Despite the extra-platelet effect of ticagrelor, it did not reduce myocardial infarct size in the present study. In STEMI patients, a 180 mg loading dose of ticagrelor might be insufficient to reduce infarct size due to the pharmacodynamic limitations of an oral agent. Further studies with higher dose or intravenous agents are necessary.
Our study has several limitations. Infarct size was measured by SPECT. However, cardiac MRI is currently used to measure infarct size because it provides superior resolution and detects subendocardial infarction as well as microvascular obstruction.13) Correlation between infarct size measured using SPECT and MRI was good, and the prognostic significance was similar between the 2 methods in patients with STEMI in previous studies.14)15) Another limitation of our study was that imaging was conducted within a very short time period after STEMI. Early SPECT imaging between 18 and 48 hours after the event often overestimates infarct size, presumably due to biochemical stunning of the myocardium, which limits isotope uptake.16) Therefore, the size of the perfusion defect in this study did not reflect true infarct size. Moreover, we did not measure serial ejection fraction or wall motion changes. Therefore, the long-term effects of ticagrelor were not demonstrated. Additionally, baseline SPECT was not performed. The difference between baseline and follow-up infarct size could be a better variable to evaluate the protective effect of ticagrelor. Furthermore, the expected sample size in the treatment group might be too small to demonstrate reduced infarct size. The SD of infarct size was unexpectedly high in both groups. Finally, the loading dose of clopidogrel was 300 mg. The lower dose of clopidogrel might have affected outcomes.
In conclusion, in a small study of STEMI patients treated with primary PCI, ticagrelor loading did not result in smaller infarct size than clopidogrel, as assessed by SPECT during the first 48 hours. Larger studies using better assessment methods for infarct size and clinical outcome evaluation are necessary to resolve this question.
 XML Download
XML Download