

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Kawasaki disease (KD), a systemic vasculitis of unknown origin, is the most common acquired cardiovascular disease in developed countries.1) Although intravenous immunoglobulin (IVIG) infusion is an effective treatment for this disease, some patients still develop coronary aneurysms.2) Giant coronary aneurysms (≥ 8 mm in diameter) account for approximately 0.5-1.0% of the total cases of KD.3) These aneurysms have a poor clinical course and can lead to occlusion or severe stenosis of the coronary artery, which can cause ischemic heart disease including myocardial infarction.4) Patients with giant aneurysms show either persistent coronary aneurysm or the development of stenosis and/or occlusion over time.5) To treat ischemic heart disease caused by KD, we have applied different types of trans-catheter and/or surgical coronary interventions, including percutaneous coronary intervention (PCI) and coronary artery bypass graft surgery (CABG). However, little is known about the long-term prognosis of patients with KD complicated by large coronary aneurysms (diameter ≥6 mm). Therefore, we conducted the present study to examine the current status, diagnosis, treatment, and prognosis of large coronary aneurysms in patients who developed a KD-related aneurysm ≥6 mm in diameter at a single institution.
Go to : 
Subjects and Methods
The medical records of 71 patients (53 men and 18 women) diagnosed with large coronary aneurysm (diameter ≥6 mm) between December 1986 and December 2013 were retrospectively reviewed from the database at Seoul National University Children's Hospital. Coronary aneurysms in all patients were diagnosed by echocardiography, cardiac computed tomography (CT), or coronary angiography. In general, follow-up examinations including physical examination, electrocardiography, and echocardiography were performed every 6 or 12 months. Follow-up coronary angiography was performed every 2 or 3 years. Pharmacological stress 99mTc-tetrofosmin scintigraphy with dipyridamole infusion was performed every 2 or 3 years. Electrocardiography during treadmill exercise was performed between the 99mTc-tetrofosmin scintigraphy. Follow-up examinations were also performed whenever patients complained of chest discomfort or other symptoms that could indicate ischemic heart disease.
We collected data on sex, age at onset, site, and size of each coronary aneurysm and/or stenosis, acute phase treatment such as IVIG, clinical course, and treatment history, including long-term medications, catheterization, and surgical interventions from patient records. In addition, we performed subgroup analysis according to the diameter of coronary aneurysm (6-8 mm vs. ≥8 mm).
This study was approved by the Institutional Review Board of Seoul National University Hospital, and informed consent was waived because of the retrospective nature of this study.
Statistical Analysis
Data are presented as ranges and the median or mean±standard deviation. From these data, we calculated the survival rate using a Kaplan-Meier analysis. We performed a Cox proportional hazards regression analysis to determine the influence of the site of coronary aneurysm, sex of the patient, and administration of IVIG on survival rate and to compare the re-intervention-free rate between two coronary aneurysm groups (6-8 mm vs. ≥8 mm). We also determined the cumulative coronary intervention rate and CABG surgery rate with Kaplan-Meier analysis. Statistical significance was considered to exist at p<0.05. All data analyses were performed with SPSS 21 (SPSS Inc., Somers, NY, USA).
Go to :
Results
Demographic findings and clinical data
The male-to-female ratio was 2.9:1 (53 male:18 female) and the mean age at KD onset was 4.6±3.3 years (range: 0.3-14.0 years). The interval of coronary aneurysm diagnosis from fever onset was 22.9±15.2 days (range: 2.0-69.0 days) and the mean elapsed time since KD onset was 12.5±6.9 years (range: 0.2-27.6 years). Five adult patients were included in this study because they showed coronary aneurysm and/or stenosis from coronary angiography similar in shape to those seen after KD, and they did not have any specific underlying cause for those coronary lesions.
We observed 46 cases (64.7%) of complete KD, 5 cases (7.0%) of incomplete KD, and 20 unclassified cases (28.3%). During the acute stage of the disease, the mean period of fever was 13.0±6.5 days (range: 4.0-40.0 days). Sixty-seven patients (94.3%) received IVIG. Patients received IVIG within a mean period of 7.6±4.6 days (range, 3.0-22.0 days). Twenty-two patients (33.8%) received one dose (2 g/kg), 11 patients (15.5%) received two doses (total dose of 4 g/kg), 8 patients (11.3%) received three doses (total dose of 6 g/kg), and 1 patient received four doses of IVIG (total dose of 8 g/kg). In addition to IVIG, 13 patients (18.3%) received intravenous high-dose (30 mg/kg) methylprednisolone pulse therapy, 1 patient received oral methotrexate, and 2 patients received infliximab infusion. Data on the total IVIG dose was not available for 27 patients (38%). These patients were patients referred from other hospitals for further treatment of coronary aneurysm after the acute stage of KD was treated or adult patients who were diagnosed with a KD-associated coronary aneurysm during coronary angiography. After the acute stage of the disease, all patients received several combinations of anti-coagulant and anti-platelet medications including aspirin, clopidogrel, and warfarin (Table 1).
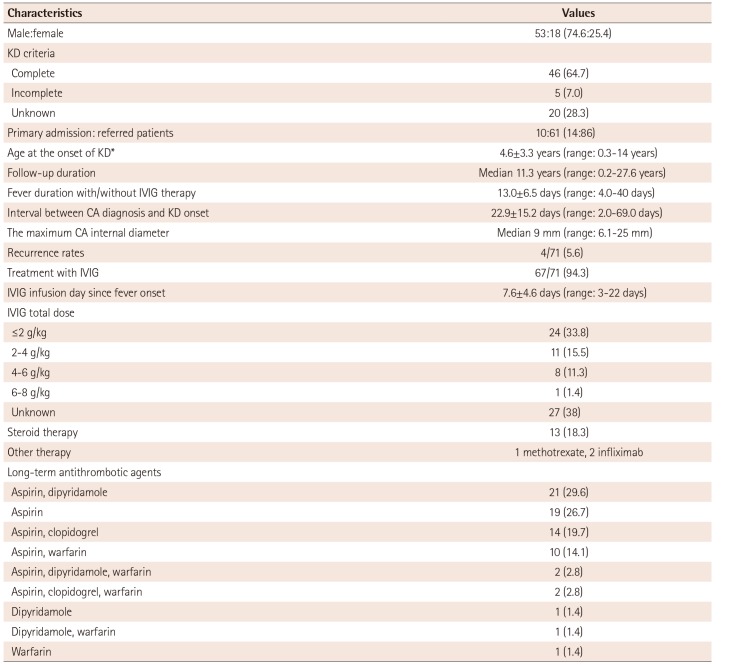
Table 1
Baseline characteristics of patients with large coronary artery aneurysm (≥6 mm)
![]()
Coronary aneurysm
The maximum coronary artery internal diameter ranged from 6.1 to 25 mm (median: 9 mm). Giant coronary aneurysm (≥8mm) occurred in 48 patients (67.6%) and large coronary aneurysm (6-8 mm) developed in 23 patients (32.4%). Coronary aneurysm progressed to coronary artery stenosis and/or complete occlusion in 30 patients (42.3%).
Coronary angiography
Primary coronary angiography was performed in 58 patients (81.7%) with a mean age of 9.8±11.1 years (range, 3.0 months to 61.0 years). The mean elapsed time from KD onset to coronary angiography was 2.0±2.4 years (range, 1.0 month to 12.0 years). Aneurysms were found in the right coronary artery (43 cases), left anterior descending artery (30 cases), left main coronary artery (4 cases), and left circumflex artery (5 cases). Of these, stenosis was found in the right coronary artery (14 cases), left anterior descending artery (10 cases), and left main coronary artery (2 cases).
Percutaneous coronary intervention
A total of 12 patients with a median age of 9.2 years (range: 4.6-17.3 years) underwent PCI. The median elapsed time between first PCI and KD onset was 5.0 years (range: 0.8-12.3 years). Procedures included percutaneous transluminal coronary-balloon angioplasty (PTCA) (9 cases) and/or stent placement (6 cases), and percutaneous transluminal coronary rotational ablation (1 case). Two patients underwent additional PCI due to restenosis. One patient underwent PTCA and stent placement twice due to restenosis and stent fracture. Four patients underwent CABG after the PCI procedure.
Coronary artery bypass graft surgery
A total of 12 patients with a median age of 15.2 years (range: 6.3-30.2 years) underwent CABG. The median elapsed time between CABG and KD onset was 8.0 years (range: 2.1-14.7 years). One patient was an acute myocardial infarction survivor. There was a single graft in 5 patients (41.7%), 2 grafts in 3 patients (25%), and 3 grafts in 4 patients (33.3%). The mean number of grafts was 1.9 per patient. Grafts were collected from the internal thoracic artery in 17 patients, the gastroepiploic artery in 4 patients, and the saphenous vein in 2 patients. The total number of grafts from all patients combined was 23. Targeted coronary arteries were the left anterior descending artery in 8 patients (42.1%), the right coronary artery in 4 patients (21%), the posterior descending artery in 4 patients (21%), the obtuse marginal artery in 2 patients (10.5%), and the diagonal branch of the left anterior descending artery in 1 patient (5.4%). The median elapsed time since CABG was 9.3 years (range: 1.5-21.0 years). One graft loss was found during post-operative follow-up.
Clinical features between two groups (coronary aneurysm 6-8 mm vs. ≥8 mm)
Patients were divided into two groups according to the size of their coronary aneurysm (Table 2, Fig. 1A). Group I consisted of 23 patients with coronary aneurysm diameter between 6 and 8 mm. Group II consisted of 48 patients with coronary aneurysm diameter ≥8 mm. Trans-catheter and/or surgical coronary interventions (mean: 1.5 interventions; range: 1 to 5 interventions) were performed in 20 patients (28.2%) from 9 months to 18 years after KD onset, resulting in a 33.7% cumulative coronary intervention rate at 20 years after KD onset. There were no differences in cumulative coronary intervention rates between the 2 aneurysm groups.

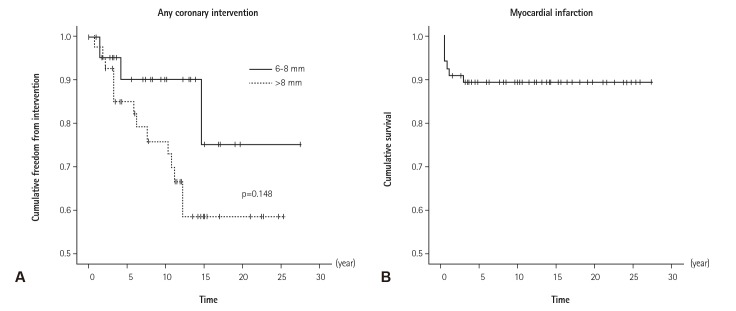 | Fig. 1Kaplan-Meier actuarial freedom from cardiac events. (A) Freedom from any intervention between coronary aneurysm size (6-8 mm vs. ≥8 mm). Trans-catheter and/or surgical coronary interventions were performed in 20 patients, resulting in a 33.7% cumulative coronary intervention rate at 20 years after KD onset. There were no differences in cumulative coronary intervention rates between two coronary aneurysm groups (p=0.148). (B) Freedom from myocardial infarction. The median elapsed time from KD onset to myocardial infarction was 3.0 months (range: 0.5-31.2 months). Cumulative survival rate was 89.6% and most myocardial infarction occurred in the first year after onset of giant coronary aneurysm. KD: Kawasaki disease.
|
Table 2
Comparison of clinical features of the CA size 6-8 mm vs. ≥8 mm groups
![]()
Patients with myocardial infarction
Among the 71 patients with coronary aneurysm diameter ≥6 mm, 7 (9.9%) experienced myocardial infarction (Table 3, Fig. 1B). Four patients presented with chest pain, 2 with dyspnea, and 1 with cardiac failure. The median age of myocardial infarction occurrence was 4.6 years (range: 2.0-8.2 years) and the median elapsed time from KD onset to myocardial infarction was 4.0 months (range: 0.5-31.2 months). Median fever duration in these patients was 9.0 days (range: 9.0-13 days). Four of the 7 patients had a complete occlusion of the coronary artery. Three patients had acute coronary artery thrombosis. There were 3 patients with two affected coronary arteries, 3 patients who had a right coronary artery infarction, and one patient had a left coronary artery infarction. Rather than differences in symptoms of coronary artery aneurysm location, younger patients presented with dyspnea and cyanosis. The main symptom in older patients was chest pain. One patient underwent CABG. One patient visited an emergency room for chest pain but died despite aggressive thrombolytic treatment and cardiopulmonary resuscitation. This patient had an 8.3 mm aneurysm in the left main coronary artery.
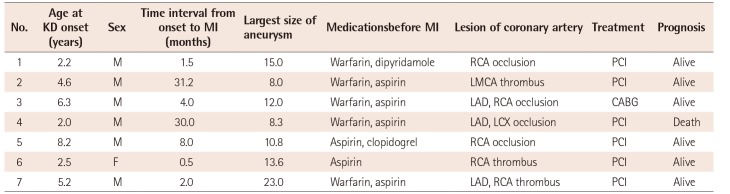
Table 3
Clinical data in patients with myocardial infarction
![]()
Go to :
Discussion
The long-term survival of patients with KD complicated by large coronary aneurysm (diameter ≥6 mm) was good in our study, despite 28.2% of patients undergoing multiple trans-catheter or surgical interventions during the 12.5±6.9 years of follow-up after KD onset. It has been >40 years since Kato et al.6) first reported the development of coronary aneurysm after acute KD, but little is known concerning the long-term prognosis of KD with giant coronary aneurysm. Suda et al.7) recently reported on the outcomes of 76 patients with giant coronary aneurysm during a 30-year follow-up period. Their study showed 59% cumulative coronary intervention rates and 88% survival rates. From a recent Korean nationwide survey of large coronary aneurysm (diameter ≥6 mm) between 1990 and 2011, severe stenosis or occlusion of the coronary artery occurred in 22% (52/239) patients during a median follow-up duration of 7.7 years (range: 2.0 months to 21.0 years) with PCI performed in 22 patients (9.2%) and CABG in 14 patients (5.8%).8) Results from these studies, along with our own findings, show that patients with large coronary aneurysm have a tendency to undergo coronary intervention, including PCI or CABG, as they increase in age.
Therefore, it is recommended that coronary angiography be routinely performed to appropriately assess patients with large sized coronary aneurysms detected on echocardiography in order to improve the chances of rehabilitating the damaged coronary artery. According to Akagi et al.,9) coronary angiography was performed in patients with coronary aneurysm with a diameter ≥4 mm present for more than six months. In our study, coronary aneurysms were first identified within a mean period of 22.9±15.2 days after KD onset and the first coronary angiography was performed at a mean elapsed time of 2.0±2.4 years (range, 1.0 month to 12.0 years) after KD onset. In comparison to the report by Akagi et al.,9) our results showed that primary coronary angiography was performed later after KD onset. Since mid-2000, we have been using cardiac CT as an initial diagnostic imaging modality to determine the severity of coronary artery aneurysm and subsequent stenosis. This may be the cause of differences in the initial timing of coronary angiography between our results and previous observation or previous report.
Echocardiography is a very useful modality for identifying coronary artery lesions and performing follow-up examinations in patients with KD.10) However, there is a possibility that sole use of echocardiography might produce false-positive or false-negative results.11) In addition, there are some cases in which it is impossible to identify a distal coronary aneurysm or stenotic lesion. Therefore, a three-dimensional imaging modality, such as cardiac CT or magnetic resonance imaging, or coronary angiography, is necessary for accurate assessment and treatment of patients with persistent moderate-to-large sized coronary aneurysm.12)13)14)
Among children with severe stenosis or occlusion of the coronary artery, there are many cases that are asymptomatic, where indications of cardiac ischemia or myocardial infarction are temporarily absent due to the development of collateral vessels and the revascularization of occluded vessels.15) However, the blood supply via these collateral vessels is unstable and may cause myocardial infarction, therefore PCI or CABG would be needed for patients with severe stenosis or occlusion of a coronary artery.16)17) As shown by Muta and Ishii18) PCI after KD onset was less efficacious compared to CABG. Our study also showed good patency of graft function after CABG.
Most cases of death due to KD occur as a result of myocardial infarction, which has high mortality.19) Giant coronary aneurysm and occlusion or severe stenosis of the coronary artery can lead to the occurrence of ischemic cardiac disease and/or myocardial infarction.20)21) Our results showed that myocardial infarction occurred in 7 patients (9.9%). All 7 patients had a giant coronary aneurysm, accompanied by the presence of coronary artery stenosis or occlusion. The median elapsed time from KD onset to myocardial infarction was 4.0 months (range: 0.5-31.2 months), even though most patients were taking warfarin before myocardial infarction. Therefore, strict control of a patient's anti-thrombotic status using combinations of anti-coagulant and anti-platelet medications for at least 3 years after KD onset is essential for patients with giant coronary aneurysm.
There was less intervention in patients with large aneurysm between 6-8 mm in diameter compared to patients with giant aneurysm (Table 2). Based on AHA guidelines, patients with large coronary artery aneurysm and giant aneurysm are in risk level IV. Although myocardial infarction only occurred in patients with coronary aneurysm ≥8 mm in diameter, there was no statistical difference in the cumulative coronary intervention rate for patients with aneurysms between 6-8 mm and those with aneurysms ≥8 mm in our study. Therefore, although the risk of major cardiac event such as MI or PCI may not be the same as that of giant aneurysms, patients with aneurysms between 6-8 mm in diameter must be carefully followed.
Another important issue for the long-term treatment of large coronary aneurysm is the follow-up system and education of young adult patients to prevent unfavorable coronary vascular remodeling. Muta et al.22) reported that general perceptions of good health are overly exaggerated, even in patients with giant coronary aneurysms and/or ischemia. These adolescent or young adult patients are easily lost to follow-up programs and stop taking their medications. Therefore, a continuous follow-up system with close cooperation between pediatric and adult cardiologists and a subsequent transition period from childhood to adult must be established to avoid losing these patients.
One limitation of this study is the retrospective nature of the study. As different treatment regimens were used during the 27-year period of our study, the treatment results cannot be taken as representative of the outcome of any single regimen. Treatment outcomes might have been better if the most current regimen had been used for all patients.
In conclusion, chances for long-term survival of KD patients complicated by a large coronary aneurysm (diameter ≥6 mm) were good even though 28.2% of patients underwent multiple transcatheter and/or surgical interventions for 12.5±6.9 years of follow-up after KD onset. Meticulous follow-up care is necessary in KD patients with coronary aneurysms 6-8 mm in diameter, with similar recommendations for patients with giant aneurysms.
Go to :
 XML Download
XML Download