

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Mechanical circulatory support is used in postoperative cases of low cardiac output condition, unresponsiveness to conventional medical care, extracorporeal cardiopulmonary resuscitation, failure of weaning from cardiopulmonary bypass, and bridge to transplantation.1)2)3)4)5)6)7)8)9) Many studies have reported on the efficacy of mechanical circulatory support, which has widespread utilization for various indications.1)2)3)4)5) However, outcomes vary among different institutions, and complication rates and mortality rates remain unsatisfactory.6)7)8) The purpose of this study was to summarize our institutional outcomes of patients who were assisted with an extracorporeal membrane oxygenation (ECMO) or a ventricular assist device (VAD) as a result of a low cardiac output in the pediatric intensive care unit (PICU). Also, we retrospectively analyzed various factors influencing survival of patients.
Subjects and Methods
Retrospective analysis was performed using data collected from 86 patients who underwent mechanical circulatory support at the Seoul National University Children's Hospital PICU unit from May 1999 to December 2014. Pediatric patients who were under 18 years of age and patients with grown-up congenital heart disease (GUCH) requiring a different approach than other adult patients for circulatory hemodynamic difference were admitted to our PICU. Eighty-six patients including 9 GUCH patients were included in our study. The total annual number of pediatric cardiac surgeries is described in Fig. 1.
A total of 78 patients used ECMO and 8 patients used VAD for mechanical circulatory support. The age of all patients ranged from 1 day to 41 years. Mean age and weight were 5.82±8.55 years and 17.79±19.93 kg, respectively. Initial mechanical circulatory support data were included for 6 patients who had had ECMO or VAD reassist during the same admission. Five (5.81%) patients diagnosed with myocarditis and 13 (15.12%) patients with dilated cardiomyopathy (DCMP) were assisted with mechanical circulatory support for medically intractable low cardiac output. In addition, 60 (69.77%) postcardiotomy patients underwent ECMO or VAD, and 8 (9.30%) patients received ECMO as rescue therapy during cardiopulmonary resuscitation (CPR). Twenty-nine (33.72%) patients received mechanical circulatory support postoperatively, while 18 (20.93%) patients were assisted without any surgery, and 5 (5.81%) patients used mechanical circulatory support before surgery. Venoarterial ECMO was used for 65 (95.59%) patients, and left VAD and Bi-VAD was needed for 2 (2.94%) patients and 5 (7.35%) patients, respectively. Twenty-six (38.24%) patients used mechanical circulatory support for under 100 hours, while 15 (22.06%) patients were assisted for over 300 hours.
This retrospective study was approved by the Institutional Review Board of Seoul National University Hospital (H-1607-182-779). The requirement for informed consent was waived.
Detailed demographic, clinical, and surgical data, including the age at assist, diagnosis, indication, laboratory results, mechanical ventilation data, mechanical circulatory support data, and complications were obtained from electronic medical records and paper chart records. Survival to discharge and late follow up echocardiography data were also analyzed.
All data were analyzed using SPSS 23.0 (SPSS Inc., Chicago, IL, USA). Descriptive data were presented as mean±standard deviation and compared by Student's t-tests. Fisher's exact test and Pearson's Chi-square analysis were used for dichotomous and categorical variables, presented as numbers with percentages. Significant variables in the univariate analysis were included in a multivariable logistic regression model. A p value less than 0.05 was considered to be statistically significant for all analysis.
Results
A total of 86 patients underwent mechanical circulatory support during the study period. ECMO was used for 78 patients and VAD for 8 patients. A single patient received VAD followed by ECMO reassist, 4 patients received ECMO to ECMO reassist, and 1 patient received ECMO to left VAD reassist. Four patients were bridged to heart transplantation after ECMO support, and 1 patient was on ECMO support before and after heart transplantation surgery. One patient was bridged to heart transplantation after VAD support (Fig. 2). In these cases, only the initial mechanical circulatory support data were included in the analysis. Forty-one (52.56%) patients were able to be weaned from ECMO and 4 (50%) patients from VAD. Survival to hospital discharge for patients with ECMO and with VAD was 28.21% and 38.50%, respectively. Overall, a total of 25 (29.07%) patients survived to discharge. Table 1 details the data for weaning and survival of mechanical circulatory support.
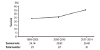
Trends for improvement in survival with the use of mechanical circulatory support over a period of 16 years are shown in Fig. 3. The survival of patients assisted increased from a survival rate of 25.00% observed from 1999 to 2010 to 35.48% from 2011 to 2014 (p=0.30).
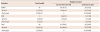
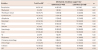
Table 2 demonstrates the demographic and clinical variables of survivors and non-survivors. Non-survivors were more likely to be neonates, under 1 month of age, and to have single ventricular physiology (p=0.03, p<0.05, respectively.). Seven patients (77.78%) out of 9 adult patients with congenital heart anomaly did not survive to discharge, and the mortality of these patients was not significantly different from pediatric patients who were under eighteen years of age (70.97%, p=0.63). A left heart problem and transposition of the great arteries were prevalent in non-survivors, whereas cardiomyopathy and myocarditis were prevalent in survivors. In spite of this, diagnosis itself was not significantly different between the 2 groups. Indications for mechanical circulatory support included post-cardiotomy, myocarditis, DCMP, and rescue therapy during CPR. Forty-six (76.67%) and 6 (75%) non-survivors were assisted with a device for post-cardiotomy and rescue therapy during CPR (Table 3). Patients diagnosed with myocarditis or DCMP who were assisted with ECMO or VAD had better survival rates. Postoperative assistance was significantly higher in non-survivors, and the average time from surgery to mechanical circulatory support was increased in non-survivors. CPR was performed in 22 (70.97%) non-survivors and 9 (29.03%) survivors prior to application of mechanical circulatory support, while CPR and CPR length showed no significant difference between the 2 groups.
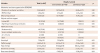
The mechanical ventilator support settings and parameters and the arterial blood gas analysis (ABGA) data before ECMO or VAD assist are described in Table 4. Survivors received a longer period of applied mechanical ventilation and had a higher mean airway pressure. Patients who did not survive to discharge required more positive end expiratory pressure (PEEP) and had a higher incidence of nitric oxide (NO) inhalation and high-frequency oscillatory ventilation. However, there was no significant difference in the duration of mechanical ventilation, PEEP, mean airway pressure, or application of inhaled NO or high-frequency oscillatory ventilation between survivors and non-survivors. Arterial blood gas test results prior to the application of ECMO or VAD were also investigated. We defined severe metabolic acidosis as a base excess lower than -10. As a result, 16 (84.21%) non-survivors and 3 (15.79%) survivors were in severe metabolic acidosis with a pH <7.2. The proportions of patients showing no ABGA abnormality were 58.97% and 41.03%, respectively (p=0.03). Moreover, significant differences were identified in arterial pH, PaO2, and base excess. PaCO2 was lower in survivors.
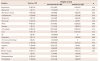
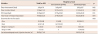
Mode, cannulation method, cannulation site, and the initial flow of mechanical circulatory support used are described in Table 5. The parameters of 4 cases of reassist were included. Survival was not associated with mode, cannulation technique, site for arterial and venous cannulation, or the location of operation performed.
The initial flow was higher in non-survivors but was not significantly different between the 2 groups. The mean duration of support was 426.19±1085.33 hours for non-survivors and 159.67±187.39 for survivors. Thirteen (86.67%) non-survivors received mechanical circulatory support for longer than 300 hours, compared to 2 (13.33%) survivors who were diagnosed with myocarditis. There was a significant difference observed in the duration of mechanical circulatory support.
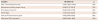
Peak serum lactate, blood urea nitrogen (BUN), creatinine, aspartate transaminase (AST), alanine transaminase (ALT), bilirubin, nadir pH, and PaO2 during assisted mechanical circulatory support were examined to determine statistically significant differences between survivors and non-survivors (Table 6). Peak serum lactate, BUN, AST, creatinine, and bilirubin were significantly higher in non-survivors than survivors, while nadir pH was lower. Nadir PaO2 was lower and peak serum ALT was higher in survivors than in non-survivors, but this result was not significant.
Overall, complications occurred in 63 out of 72 patients and 47 out of 48 non-survivors. Those who failed to survive were significantly more likely to suffer complications compared to survivors, according to the detailed information in Table 7. Thrombus found in circuit occurred significantly more frequently in survivors, whereas neurological problems, hemorrhage, and infection occurred significantly more frequently in non-survivors. In our study, the prevalence of cardiovascular complication, arrhythmia, renal complication, and hematological complication such as intravascular hemolysis, GI problems, respiratory problems, and pulmonary hemorrhage were higher in non-survivors, although without significance.
All patients who received mechanical circulatory support over 250 hours had complications, but 87.5% of patients supported for less than 250 hours had complications. According to Table 8, prolonged use of mechanical circulatory support, over 250 hours, is related to higher risks of complications, such as neurologic problems, hematologic problems, hemorrhage, and infection.
Associated variables determined by univariate analysis were analyzed by multivariable logistic regression (Table 9). PaO2 under 100 mmHg before assistance, postoperative assistance, neurological complications, hemorrhage, peak serum bilirubin level, and AST level during assistance were all predictors of hospital mortality.
Table 10 summarizes days of chest opening, days intubated, the length of stay in the ICU, and the total length of hospital stay. Survivors stayed significantly longer in the hospital compared to non-survivors. Twenty-two (25.58%) patients survived after the first assist, and 20 (90.91%) of these patients survived to discharge. Five patients were bridged to transplant, and 4 survived to discharge. Two patients were successfully weaned and sustained sufficient cardiac output but expired in the same admission period. The mean ejection fraction examined in the last echocardiography was 59.55±17.46%.
Discussion
Mechanical circulatory support has been widely used in the treatment of low cardiac output patients, and many recent studies have reported its outcomes.1)2)3)4)5) However, clinical indications, definite predictors for mortality, and guidelines remain to be established due to inconsistencies in results and insufficient accumulated cases.6)7)8) The aim of this study was to report our experiences with patients placed on ECMO or VAD in the PICU and to determine the variables associated with hospital mortality. The survival of low cardiac output patients, who would struggle to survive without any additional support, was about 29%. In addition, 52% of patients could be disconnected from the mechanical circulatory assist device.
This data is consistent with previously published data concerning ECMO.3)5)6)8) We included the data of 8 VAD deployed patients in a group study. Despite the fact that the total number of VAD deployed patients was too small to make the result reliable, 50% could be weaned from VAD and 37.5% of patients survived, similar to the results of ECMO.
We found that mortality rate follows a decreasing trend and has been reduced by over 10% since 2010. The necessity of improving such devices to increase the survival rate and reduce the complication rate has been demonstrated since many studies have reported the effectiveness of ECMO and VAD.9)10) Not only upgraded devices, such as the use of centrifugal pumps, the percutaneous cannulation technique, and heparin-coated circuits, but ICU systems with accumulated experience also contribute to improved outcomes.11) In addition, 3 out of 4 successful heart transplantation surgeries after running ECMO or VAD as a bridge were performed after 2010 in our study. Heart transplantation could be a contributing factor of increasing survival after 2010. In the same context, we expect that long-term VAD will play a role in the treatment of patients with low cardiac output and those waiting for a donor transplant. Lower complication rates and longer duration of assistance of long-term VAD, compared to ECMO, make decreased mortality rates a possibility. Consistent with previous reports,8)12) neonates under 1 month of age and single ventricle physiology patients were more vulnerable to death. This indicates that careful decision making and thoroughly confirming a patient's condition, as well as expecting benefits from the assistance, are required, especially for neonates and single ventricle patients prior to applying mechanical circulatory support.
The anatomic diagnosis or indication for mechanical circulatory support did not make a difference in terms of patient survival. However, patients with a left heart lesion, double outlet right ventricle, and transposition of the great vessels were less likely to survive. As ECMO and VAD do not provide total substitution of the circulatory system, it is more difficult to fulfill insufficient circulation in patients with complex cardiac anomalies. Furthermore, we found that patients who had undergone cardiotomy were at an increased risk of hospital mortality compared to patients with myocarditis and DCMP. Previous studies have outlined this tendency of cardiac surgery, causing a further decline in cardiac function and a systemic inflammatory reaction after surgery worsening the systemic condition.13) In contrast, improved survival is expected in myocarditis and DCMP for the use of ECMO or VAD as a bridge to recovery or heart transplantation.14) Aggressive use of mechanical circulatory support for DCMP and myocarditis with intractable low cardiac output can be considered.
Metabolic acidosis before and during ECMO has been reported as a risk factor of hospital mortality.8)15) Consistent with previous studies, pre-ECMO/VAD arterial pH, PaO2, and base excess were related to survival. Severe metabolic acidosis, low arterial pH, and PaO2 indicate inadequate circulation, which could cause critical complications and death. Mechanical circulatory supply may be insufficient to reverse organ dysfunction already in progress. The central nervous system could already be damaged in patients with severe metabolic acidosis with low PaO2 and arterial pH.16) Therefore, it is necessary to closely monitor the acid-base status of high-risk patients to decide upon early mechanical circulatory support insertion before irreparable organ damage.
Many studies have reported the association between mortality and laboratory results at 24 or 48 hours after deploying ECMO.9)17)18) We retrospectively analyzed the peak and nadir of chemical indicators. Serum AST and bilirubin were predictive factors of death for ECMO or VAD. The results suggest that not only persistent metabolic acidosis, but also various laboratory findings that imply a progression of multiorgan failure can be good candidates for mortality markers. Furthermore, continuous follow up of chemical indicators to update nadir and peak values may be necessary because these patients are at a high risk of complication and death.
Over 250 hours of ECMO support was not recommended in previous research.8) We did observe that there was a negative exponential distribution of the categorical duration of ECMO or VAD support and the number of survivors. The proportion of non-survivors with assistance of mechanical circulatory support over 250 hours was significantly higher. Moreover, survivors who were assisted for over 250 hours were diagnosed with myocarditis and used ECMO or VAD as a bridge to recovery. We believe that prolonged use of mechanical circulatory support for more than 250 hours in postcardiotomy patients could predict hospital mortality and higher risk of critical complications, such as neurological problems, hematologic problems, hemorrhage, and infection.
Complication rates were found to be related with survival to discharge. Renal, hematologic, and liver complications occurred in over half of all studied patients, and renal failure was diagnosed in two-thirds of non-survivors. Infection, neurological problems, and hemorrhage were significant predictors of poor outcome, which could be caused by long-term use of mechanical circulatory support and abnormal coagulation systems.19) Survivors with complications normally stayed longer in the hospital than survivors without complications. Meticulous attention to patients and prepared management of known complications can be beneficial for early diagnosis, treatment, and survival without sequelae.15)
There were several limitations to this study. First, patient selection was limited as our study was a retrospective, observational, single-center study. Second, missing data limited the use of many variables for analysis. Significantly associated variables could have been excluded for our analysis. Third, the predictive power of significant variables was not satisfactory due to the small sample size.
Currently, mechanical circulatory support is widely used for cardiopulmonary support in various indications, including postcardiotomy, rescue therapy after CPR, DCMP, and myocarditis. In our center, 52.33% of patients were able to be weaned from ECMO or VAD. Before 2010, 25% of patients who were assisted survived, and 35.48% of patients who assisted after 2010 survived, which implies an improvement in outcome. The age of the patient and a single ventricle physiology were more associated with mortality than the indication and anatomical diagnosis. Informed consent for guidance and careful decision regarding deployment are required. Reduced outcomes were expected after postoperative assistance compared to nonsurgical assistance, but earlier assistance after surgery is recommended. The acid-base status of patients not only before the assistance, but also during the assistance was a strong determinant of mortality. Also, large increases in serum BUN, creatinine, AST, and bilirubin during ECMO or VAD, indicating multiorgan failure, were possible predictors of death. Longer duration of assistance, especially over 250 hours, increased the chances of a bad prognosis, except in cases using ECMO or VAD as a bridge to recovery or transplantation. High complication rates have been a problem.20) Neurological problems and hemorrhage were associated with a greater chance of mortality. Better strategies including early diagnosis, aggressive but meticulous management, and a multimodality approach are required to improve survival rates, lengthen hospital stay, and reduce sequelae in survivors.21)






 XML Download
XML Download