

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Chronic kidney disease (CKD) is not uncommon in patients with coronary artery disease (CAD), and it affects up to 25% of patients that require coronary revascularization.1)2)3)4) CKD is an independent predictor of mortality among patients with significant CAD,5)6) and multiple coronary arteries are often involved in these patients.7) Both percutaneous coronary intervention (PCI) with drug-eluting stents (DES) and coronary artery bypass grafting (CABG) have been used as effective revascularization therapies for patients with multivessel CAD. In general, CABG when compared with PCI is associated with improved clinical outcomes in high-risk patients with multivessel CAD.8)9)10)11) However, these studies were predominantly performed in the era of bare-metal stents, and patients with CKD were excluded from participating in the majority of clinical trials. Therefore, the optimal revascularization strategy for CKD patients with multivessel CAD remains unknown. In this study, we compared long-term PCI outcomes with DES versus CABG in a large sample of patients with CKD and multivessel CAD.
Subjects and Methods
Study population
The Asan Multivessel Registry is a single-center, prospective study designed to evaluate the treatment effects of PCI with DES and CABG for multivessel CAD.12)13) Briefly, this registry involves a prospective, single center recruitment of patients with multivessel CAD who received PCI with DES or isolated CABG at the Asan Medical Center (Seoul, Korea) between January 2003 and December 2013. Patients with a history of prior CABG, those who underwent concomitant valvular or aortic surgery, and those who had experienced an acute myocardial infarction (MI) within 24 h before revascularization or presented with cardiogenic shock were excluded. Among these patients, 2108 consecutive patients with CKD and multivessel CAD who underwent PCI with DES (n=1165) or CABG (n=943) were identified. The present study was approved by the local institutional review board.
PCI was performed according to current practice guidelines.14) The specific type of DES was selected based on the operator's discretion. Antiplatelet therapy and periprocedural anticoagulation followed standard regimens. Following the procedure, patients were prescribed aspirin indefinitely and clopidogrel for at least 6 months, regardless of DES type.12) Surgical revascularization was performed using standard bypass techniques; whenever possible, the internal thoracic artery was preferentially utilized for revascularization of the left anterior descending artery.15)
Definitions and study outcomes
The primary outcome was a composite of mortality from any cause, MI, or stroke. The secondary outcomes were individual components of primary outcome and repeat revascularization. The diagnosis of acute MI was defined as either complications at the index admission (defined as new pathologic Q waves after index treatment) or follow-up MI requiring subsequent hospitalizations (defined as an emergency admission with a principal diagnosis of MI), as described previously.16) Stroke, as indicated by neurological deficits, was confirmed by a neurologist based on imaging studies. Repeat revascularization included target vessel revascularization and non-target vessel revascularization. In the PCI group, stent thrombosis was defined as definite or probable events, according to the Academic Research Consortium classification.17) CKD was defined as an estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2, which was calculated using the modification of diet in renal disease equation for at least three months.18)19) The renal replacement therapy (RRT) group was defined as patients that received hemodialysis or peritoneal dialysis.
Clinical, angiographic, procedural or operative, and outcome data were prospectively recorded in the dedicated PCI and surgical databases by independent research personnel. Clinical follow-up was performed at one month, six months, and one year, and subsequent follow-up was performed annually by either office visit or telephone.
Statistical analysis
Continuous and categorical covariates were summarized as the mean±standard deviation or the count (%). Baseline variables of the patients between the two treatment groups were compared with the t test or Wilcoxon rank-sum tests for continuous variables and with the chi-square statistics or Fisher's exact test for categorical variables. Survival curves were constructed using Kaplan-Meier estimates and were compared with the log-rank test. Unadjusted and adjusted Cox proportional hazard models were used to assess the long-term rates of clinical outcomes between the two treatment strategies among the total population and subgroups. Covariates that were statistically significant on univariate analysis and/or those that were clinically relevant were considered as candidate variables in the multivariate models. Adjusted covariates included age, hypertension, diabetes mellitus, dyslipidemia, history of myocardial infarction, stroke, peripheral arterial disease, heart failure, history of PCI and CABG, extent of CAD, involvement of left main coronary artery, presence as acute coronary syndrome, and treatment strategy. In the Cox model, the proportionality assumptions were assessed by the Schoenfeld residual test and no relevant violations were detected. All reported p-values are two-sided, and p values<0.05 were considered statistically significant. Analysis was performed with SPSS software, version 21.0 (SPSS Inc., Chicago, IL, USA).
Results
Baseline characteristics
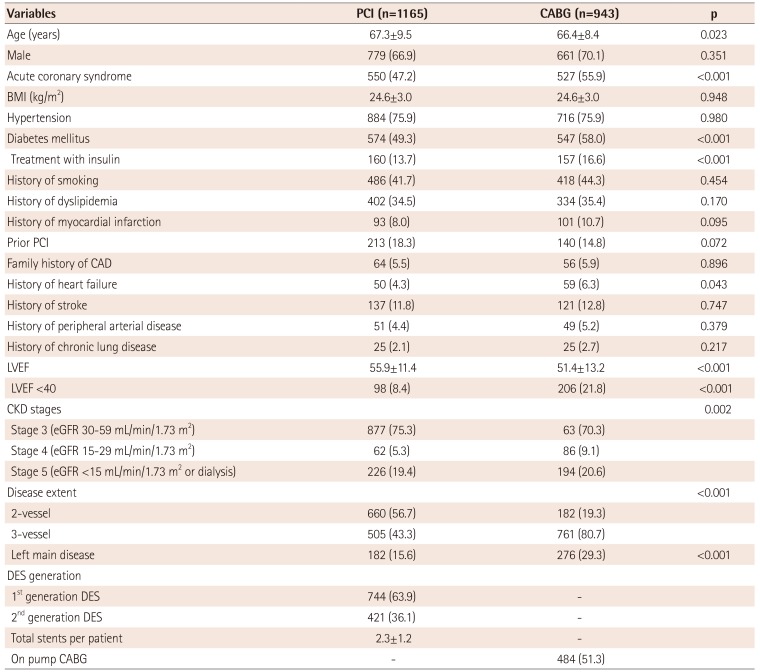
The mean age of the patients was 66.9 years, 68.3% of the patients were men, and 1121 (53.2%) patients had diabetes mellitus. Baseline characteristics of patients according to treatment strategy are shown in Table 1. The results indicated that patients who received PCI were younger, had a lower incidence of diabetes mellitus, history of heart failure, and three-vessel disease, and had a higher incidence of left main disease compared with CABG patients. The number of implanted stents per patients was 2.3±1.2 in the PCI group, and the number of grafts used was 2.9±1.0 in the CABG group.
Clinical outcomes
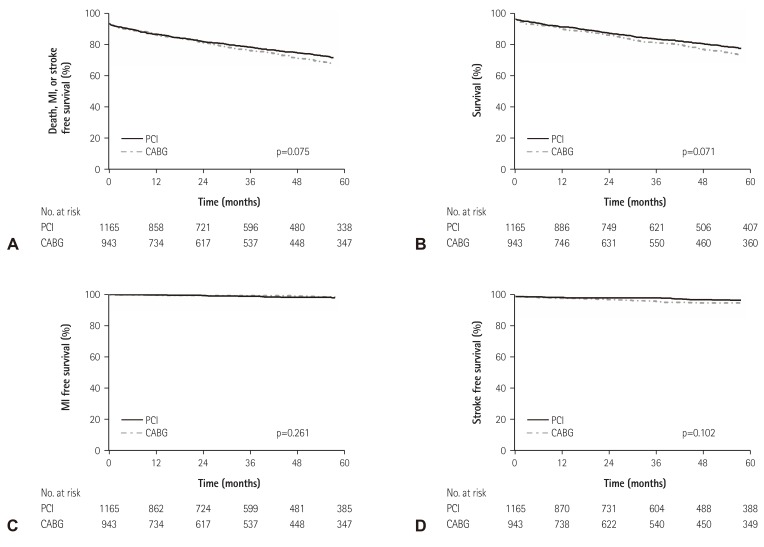
During the 41.4-month follow-up period (interquartile range, 12.175.5 months), primary outcomes occurred in 307 (26.4%) patients in the PCI group and 304 (32.2%) patients in the CABG group (hazard ratio [HR], 0.866; 95% confidence interval [CI], 0.739-1.015; p=0.076). The Kapan-Meier curve did not show a significant difference in primary outcomes up to 1 year (p=0.839) and up to 5 years (p=0.075) between the PCI and CABG groups. In unadjusted analysis, the risks of all-cause mortality, MI, or stroke were similar between the two treatment strategies, whereas repeat revascularization was increased in PCI patients (Table 2).
Adjusted analysis also demonstrated that there were no significant differences in the cumulative incidence of primary outcomes (adjusted HR, 0.941; 95% CI, 0.791–1.120; p=0.493), all-cause mortality (adjusted HR, 0.907; 95% CI, 0.765–1.089; p=0.295), or stroke (HR, 0.926; 95% CI, 0.569–1.607; p=0.758) between the two treatment strategies. However, PCI was associated with higher risks of repeat revascularization compared with CABG (adjusted HR, 4.718; 95% CI, 3.198–6.959; p<0.001, Table 2, Fig. 1).
Subgroup analysis
Survival curves were created with Kaplan-Meier estimates in various subgroups to determine whether the non-significant effect observed for the treatment strategy in the overall population was consistent. There were no significant differences in the rates of primary outcome, mortality, MI, or stroke up to 1 and 5 years between the two treatment strategies among patients receiving hemodialysis or peritoneal dialysis (Table 3, Fig. 2). Similarly, no significant differences in the cumulative incidence of primary outcomes up to 1 and 5 years in patients with three-vessel disease, diabetes mellitus, or left ventricular ejection fraction less <40% were detected (Fig. 2).
Discussion
Among patients with CKD and multivessel CAD, the risks of a composite outcome of mortality from any cause, MI, or stroke were similar between the PCI and CABG groups, whereas PCI was associated with a higher risk of repeat revascularization. These findings were consistent in major clinical subgroups, including RRT, three-vessel disease, diabetes mellitus, or decreased LV function.
CKD represents an important high-risk subgroup of patients undergoing revascularization.2)3)4)9) PCI in patients with CKD is associated with a higher risk due to its increased incidence of repeat revascularization, acute renal failure, and mortality.1)2)20) In addition, patients with CKD have a poor prognosis after CABG, as CKD is associated with increased postoperative bleeding rates, longer postoperative mechanical ventilation time, and increased hospital stay.3)4)21) As CKD progresses, some patients exhibit chronic renal failure and these patients should receive RRT, but limited data are available on the prognosis of RRT patients with CAD.
Several studies have compared PCI and CABG in patients with multivessel CAD. Early studies have demonstrated that long-term clinical outcomes were equivalent in patients who underwent PCI or CABG, although the subsequent revascularization rate was significantly higher in the PCI group.22)23) In the bare metal stent era, PCI with bare metal stent or balloon angioplasty and CABG for multivessel CAD exhibited similar rates of mortality and a composite of mortality or MI; however, CABG demonstrated a survival advantage in patients with diabetes or older patients.24) In the DES era, the FREEDOM trial showed that CABG was superior to PCI with DES in that CABG significantly reduced mortality rates and MI in patients with diabetes and multivessel CAD.25) Likewise, CABG, as compared with PCI with DES, significantly reduced the long-term risk of mortality in nondiabetic patients with multivessel CAD.26) Therefore, in the DES era, despite advances in stent technology, CABG demonstrated improved clinical outcomes of mortality in patients with multivessel CAD compared to PCI,25)26)27) supporting the hypothesis that CABG is the preferred strategy for the majority of patients with multivessel CAD.
CKD is a poor prognostic factor of mortality or morbidity after revascularization with PCI or CABG,1)2)3)4)9) and some studies reported that PCI with DES showed comparable results when compared with CABG in patients with multivessel CAD and CKD.28)29) In the present study, which included >2000 patients with CKD and multivessel CAD, there were no significant differences in the risk of primary outcomes, mortality, MI, or stroke between the two treatment strategies, and PCI was associated with an elevated rate of repeat revascularization. Similarly, in patients with RRT, there were no significant differences in the rates of primary outcomes, mortality, MI, or stroke between the two treatment groups. In addition, among CKD patients with other risk factors, such as three-vessel disease, diabetes mellitus, or decreased left ventricular dysfunction, there were no significant differences in the occurrence of primary outcomes. Our findings are consistent with those of a recent report, showing that PCI is associated with a similar long-term risk of death compared with CABG in patients with CKD and multivessel CAD.30) Altogether, PCI and CABG are similar in hard clinical outcomes for patients with CKD and multivessel CAD, suggesting that PCI with DES is a safe and effective in treating such patients.



 XML Download
XML Download