

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Appropriate use criteria (AUC) were developed to monitor the use and improve the quality of percutaneous coronary intervention (PCI) in the United States in 2009,1) and updated in 20122) and 2016.3) Since the first publication of AUC for coronary revascularization, there have been significant reductions in the proportion of PCI classified as inappropriate.4) However, these criteria are difficult to apply to Korean practice considering differences in the practice environment and healthcare system in the country.5)
Once developed, the AUC need to be tested in a nationwide database. The CathPCI registry was a founding member of the National Cardiovascular Data Registry (NCDR), which represents one of the most important efforts to monitor the quality of PCI practice since 1997.6) The utility of the CathPCI registry lies in its comprehensive scope, encompassing treatment monitoring, quality improvement, clinical research, and support for guideline developments. The Korea PCI (K-PCI) registry is the first nationwide PCI registry in Korea for the same purpose.
In this study, we developed Korean AUC reflecting the current Korean practice pattern and tested them in a nationwide database. We hope that this Korean AUC will be utilized for development of improved tools for PCI quality monitoring. Thus, the purpose of this study was to develop criteria for the Korean PCI practice pattern (KP3) and to analyze the K-PCI registry based on the developed criteria.
Materials and Methods
Study population and variables
The K-PCI registry is a retrospective multicenter registry of patients with coronary artery disease who underwent PCI. From January 2014 through December 2014, all consecutive patients were enrolled from 92 high volume coronary intervention centers in Korea.
This was an all-comer study with no exclusion criteria. The local Institutional Review Board at each center approved this study. Informed consent was waived at all centers, considering the study's retrospective enrollment without clinical follow-up design. Data were collected using a web-based reporting system.
This study was directed by the Korean PCI Registry Committee (co-directed by Dr. Hyo-Soo Kim and Dr. Hyeon-Cheol Gwon), and co-sponsored by the Korean Society of Cardiology and the Korean Society of Interventional Cardiology.
Development of the algorithm for Korean PCI practice pattern and study endpoint
The Korean PCI practice pattern (KP3) algorithm was determined in consensus meetings attended by members of the Korean PCI Registry Committee. The key algorithm was adopted from the ‘AUC for coronary revascularization developed by ACCF/SCAI/STS/AATS/AHA/ASNC/HFSA/SCCT’2, which was modified with consideration for the Korean healthcare system and environment (Supplementary Data in the online-only Data Supplement).
First, for cases of acute coronary syndrome (ACS) defined as unstable angina or myocardial infarction, we developed possible indications for PCI using six clinical components of patients presenting with ACS: [1] clinical presentation (e.g., STEMI, NSTEMI, unstable angina), [2] evidence of cardiogenic shock upon arrival, [3] administration of fibrinolytic therapy, [4] evidence of heart failure, persistent or recurrent ischemia, hemodynamic instability, or unstable ventricular arrhythmia, [5] time of initial presentation (≤12 hours vs. >12 hours), and [6] high risk features associated with NSTEMI or unstable angina. As a result, we developed 9 indications for PCI in ACS treatment. We then rated each indication as KP3 class A, B, or C. KP3 class A was defined as the strategy evidenced by many randomized trials and/or more conservative for PCI rather than medical therapy or coronary artery bypass surgery. KP3 class C was defined as the strategy less evidenced by randomized trials and/or more aggressive for PCI compared to medical therapy or coronary artery bypass surgery. Class B was partly class A and partly class C with conflicting evidence and/or a divergence of opinions among the committee members.
Second, for cases of stable non-ACS, we developed possible indications for PCI using five clinical components of stable CAD patients: [1] severity of ischemic symptoms (asymptomatic, Canadian Cardiovascular Society [CCS] Class I or II vs. III or IV), [2] extent of anti-ischemic medical therapy (none vs. one or more classes of anti-anginal therapy), [3] results of noninvasive or invasive supportive tests including IVUS and FFR (not done/negative test: low-risk findings vs. positive test: high-risk findings), [4] prior history of bypass surgery, and [5] extent of coronary disease (1-, 2-, 3-vessel disease, with or without proximal LAD, CTO, or left main stenosis). As a result, we developed 38 indications for PCI in the treatment of non-ACS patients (Supplementary Data in the online-only Data Supplement). We then rated each indication for PCI for non-ACS patients as KP3 class A, B, or C depending on the presence and severity of angina-related symptoms. Angina-related symptoms were defined according to CCS classification.
The KP3 algorithm was designed to describe nationwide PCI practice patterns for cases involving the preferential use of PCI over medical treatment or coronary artery bypass graft (CABG), but was not designed to examine the suitability of individual PCI cases.
Statistical analysis
Statistical analysis was performed independently in collaboration with Duke University, USA. Continuous variables are presented as medians with interquartile ranges (IQRs), and categorical variables are presented as numbers (percentages). Continuous variables were compared using Student's t-test or the Wilcoxon rank-sum test. Categorical data were evaluated using the Chi-square test. All p values were two-tailed. A p value<0.05 was considered statistically significant.
Results
Study population
From January 2014 through December 2014, 44967 consecutive patients were enrolled from 92 high volume coronary intervention centers out of a total 150 intervention centers currently operating in Korea. Three of 92 centers failed to submit all patients in the registry.
Baseline clinical and procedural characteristics
Baseline clinical and angiographic characteristics, procedural details, and in-center outcomes will be reported in a separate paper in the Korean Circulation Journal. Briefly, the proportion of male patients was 70.3%, and the median age of all patients was 66.0 (IQR 57.0-74.0) years. Diabetes was found in 35.9% of patients, renal failure in 6.4%, prior myocardial infarction in 9.2%, prior PCI in 24.0%, prior CABG in 1.3%, prior cerebrovascular disease in 8.8%, and peripheral artery disease in 2.7%. The distribution of clinical diagnoses was as follows: silent ischemia 3.5%, stable angina 22.6%, unstable angina 35.9%, non-ST elevation myocardial infarction 19.7%, and ST-elevation myocardial infarction 18.4%. Cardiogenic shock was noted in 3.1% of patients and cardiac arrest in 2.3% of patients. A noninvasive test before PCI (including treadmill test, thallium SPECT, stress echocardiography, and stress magnetic resonance imaging) was performed in 13.9% of patients (9.8% in ACS patients and 25.8% in non-ACS patients). Multivessel disease was noted in 66.3%, left main disease in 4.9%, and proximal LAD lesion in 31.9% of patients. PCI was performed electively in 66.7% of patients, and was otherwise performed as an urgent or emergent procedure. A drug-eluting stent was used in 91.3% of patients, a bare metal stent in 1.1%, and balloon angioplasty in all other cases.
Distribution of classes of Korean PCI practice pattern
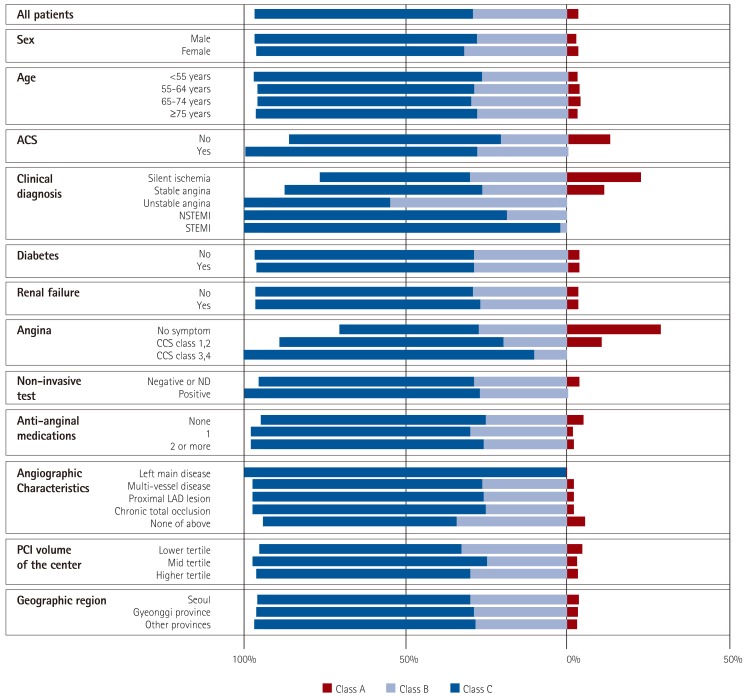
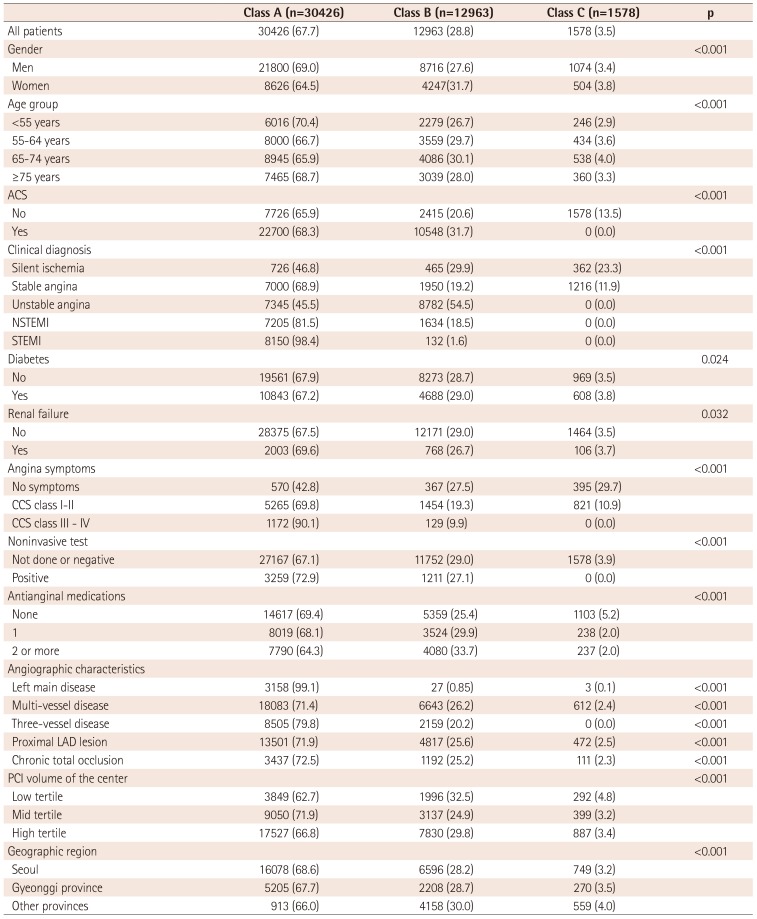
Korean PCI practice pattern (KP3) class A was noted in 67.7%, class B in 28.8%, and class C in 3.5% of cases (Table 1, Fig. 1). The distributions of KP3 classes were significantly different according to demographic, clinical, and angiographic variables (Table 1, Fig. 1). Notably, class A was found more frequently in patients with ACS, while class C was more common in non-ACS patients (p<0.001), noted in 13.5% of the patients. Class C was noted in 29.7% of asymptomatic patients, in 10.9% of patients with mild chest pain (CCS class I or II), and in 0% of patients with severe chest pain (CCS class III or IV). Regarding angiographic characteristics, class C was noted in a small proportion of patients with complex coronary artery diseases such as left main disease, multi-vessel disease, or chronic total occlusion.
Proportion of class C patients in the centers
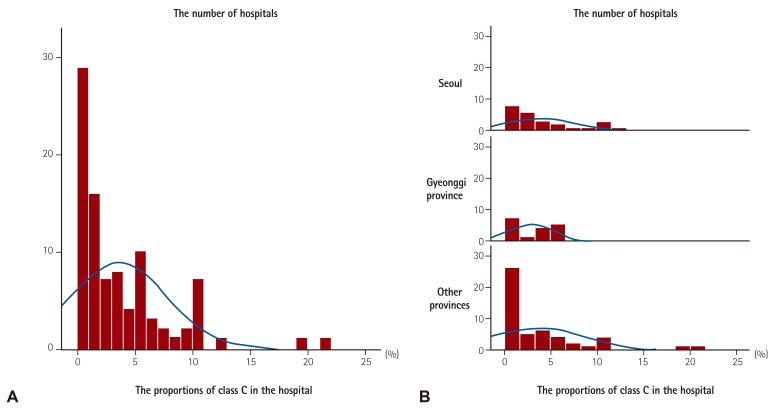
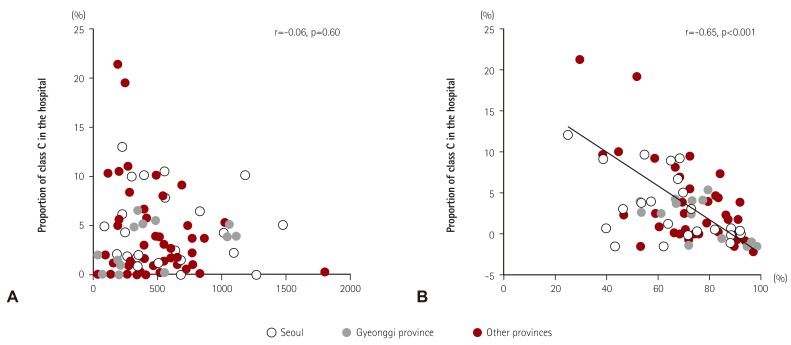
The median proportion of class C cases in all centers was 2.0% (interquartile range 0.5-5.2%) (Fig. 2). A greater than 15% proportion of class C cases was noted only in two centers, while a proportion less than 1% was noted in 29 centers. The proportion of class C cases found in the hospital setting was less variable in Seoul and Gyeonggi province (which is the nearest province to Seoul) (Fig. 2B). The proportion of class C cases was not dependent on the number of PCIs performed per center (r=-0.06, p=0.601, Fig. 3A). The initial diagnosis of ACS was significantly associated with the proportion of class C cases found in a given center (r=-0.65, p<0.001, Fig. 3B).
In-hospital clinical outcomes according to KP3 class
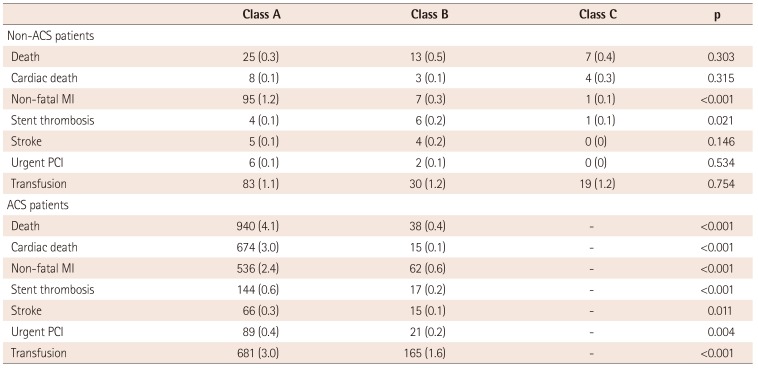
In-hospital clinical outcomes were similar among the three KP3 classes in non-ACS patients, whereas they were significantly different in ACS patients (Table 2). However, there were no signs of worse in-hospital outcomes in class C patients.
Discussion
The aim of this study was to develop the Korean PCI practice pattern (KPPP, KP3) and apply it to a nationwide database of PCI cases. The key findings were as follows: 1) KP3 class A was noted in 67.7% of patients, class B in 28.8%, and class C in 3.5%, 2) the median proportion of class C was 2.0% of patients (IQR 0.5-5.2%), and 3) the distribution of KP3 classes varied significantly depending on clinical, angiographic, and procedural characteristics. KP3 class was mainly determined by the severity of angina-related symptoms and the diagnosis of ACS. For example, the same procedure would be categorized as class A in the case of symptomatic ACS, while it would be categorized as class C in the case of less symptomatic, stable CAD. 4) The proportion of KP3 class C cases in each intervention center was not dependent on PCI volume, but on the proportion of ACS cases.
American guidelines recommend the participation of interventional centers in a regional or national PCI registry for the purpose of benchmarking outcomes against current national norms. The CathPCI registry has been developed as a nationwide registry by the American College of Cardiology in the United States as previously described.7) Sweden and other European countries have also developed nationwide registries of PCI, established either by academic societies or the government.8)9) The Korea percutaneous coronary intervention (K-PCI) registry is the first nationwide PCI registry in Korea, established as a joint effort of the Korean Society of Cardiology and the Korean Society of Interventional Cardiology.
Appropriate use criteria (AUC) were developed based on the CathPCI registry, which was built to document cases involving PCI. However, it is challenging to apply these criteria to Korean practice considering the different practice environment in Korea, as well as the different database structure of the K-PCI registry. When the AUC were applied in Japan, the differences between the two countries were acknowledged, and local discrepancies of practice were considered.10) In this study, we adopted key algorithms from the ‘AUC for coronary revascularization’ developed by American academic societies2) and revised them to reflect Korean contemporary practice in consensus meetings of the members of the Korean PCI Registry Committee.
The clinical practice environment in Korea is different that of the US or European countries, and this influences the decision for diagnostic study and/or revascularization in real-world practice. For example, medical costs associated with physicians and invasive studies are relatively low in Korea, while those associated with noninvasive studies were relatively high. The use of drug-eluting stents was consistently high in Korea, and Korean real-world data reported excellent safety and short- and long-term outcomes associated with PCI, especially with second-generation drug-eluting stents.11) When considering the applicability of the Korean practice pattern algorithm, the incorporation of results from noninvasive risk stratification, symptoms, medication status, and extent of coronary disease as assessed by angiography was modified (Supplementary Data in the online-only Data Supplement). The purpose of the algorithm of the Korean PCI Practice Pattern was to describe nationwide distributions of PCI practice patterns for cases involving the preferential use of PCI over medical treatment or CABG, and not to examine the suitability of PCI for individual cases. Practice pattern reporting involves the largest, voluntary, nationwide studies in order to properly document the differences and heterogeneity of PCI usage in Korea by Korean medical professional societies. This report should be the basis for efforts to develop Korean standards for the use of PCI. Further studies are needed to fill the gaps in clinical evidence and to improve ischemic heart disease outcomes.
Most patients were categorized as KP3 class A or B, and only 3.5% of patients were categorized as class C. The distribution of the classes was found to be significantly influenced by all of the important clinical and angiographic variables, partly due to the number of cases. A diagnosis of ACS and angina-related symptoms as measured by CCS class seem to be the most influential variables for determining KP3 class. These results contradict prior reports. Although the vast majority of PCI performed in acute settings was classified as appropriate using the standardized AUC from the US NCDR CathPCI registry, approximately 12% of procedures performed in a non-acute setting were classified as inappropriate.12) A total of 221252 non-acute procedures were classified as inappropriate because physicians performed PCI more commonly in men, in Caucasian patients, and in those with private insurance.13) They also found that those admitted to rural hospitals were less likely to undergo inappropriate PCI than those treated at suburban hospitals. In our study, the median proportion of class C cases per center was 2.0%, and this proportion was more than 15% in only two centers. The proportion of class C cases was not correlated with PCI volume, but the distribution of class C cases in each interventional center was highly dependent on the proportion of patients with ACS and severe symptoms.
We think the current general practice pattern abides mostly by the current guidelines and expert consensus. The proportion of classes must have been influenced by the algorithm of KP3 classification system, but these numbers will be reference values for development of future AUC criteria in Korea. Therefore, these results should be interpreted very carefully when applied to a specific center or operator, considering the complex relationships between the variables. Moreover, the in-hospital clinical outcomes were not worse in patients categorized as class C. Long-term outcomes according to KP3 class should be analyzed in future studies. Therefore, the KP3 class system should not be utilized as a guide for reimbursement.14)
It is notable the class C was found mostly in non-ACS patients (patients with silent ischemia and stable angina). Also, noninvasive tests seem to be underutilized in this Korean population. Investigation into the proper utilization of noninvasive tests in non-ACS patients with cost-benefit assessment in the Korean healthcare system is warranted.
Limitations of this study
The K-PCI registry is the largest PCI registry in Korea and includes most patients from the high volume centers in Korea. This study, however, has several limitations. 1) This study did not enroll all patients who underwent PCI in Korea and the results represent only those patients treated in high volume centers in Korea. 2) This study used a retrospective registry rather than a prospective registry. Therefore, definitions of certain variables might vary from center to center, although we provided strict definitions for all variables before patient enrollment. On-site monitoring was conducted in a small number of centers, and not all cases were monitored for the accuracy of reports given to our team of researchers. 3) The algorithm of Korean PCI practice pattern was designed by members of the Korean PCI Registry Committee who modified the AUC used in the United States through expert consensus. The external validity of these criteria has not yet been determined and must be the subject of future analysis.
Conclusion
We report the current PCI practice pattern in Korea using the new Korean PCI practice pattern algorithm through analysis of a nationwide, real-world PCI registry. The results of this study should be interpreted carefully with due regard to the complex relationships between the determining variables and the insurance and healthcare systems in Korea. This study provides background to develop the ‘Korean Appropriate Use Criteria for PCI,’ ultimately aiding in the development of rational guidelines and administrative policies for the use of PCI in Korea.
 XML Download
XML Download