

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Congenitally corrected transposition of the great arteries (ccTGA) is a rare disease that is characterized by atrioventricular and ventriculoarterial discordance.1) Although the blood circulation is physiologic because of the combination of duplicated discordances, systemic ventricular dysfunction develops frequently because the systemic circulation is supported by a morphologic right ventricle (mRV). Chronic systemic pressure overload increases wall stress in the mRV, which results in myocardial hypertrophy and ischemia, and eventually abnormal regional myocardial function in the third or fourth decade. Systemic ventricular dysfunction can also be caused by volume overload such as tricuspid regurgitation (TR) and associated shunt lesions.
The classical physiologic (or conventional) repair is directed toward the associated cardiac anomalies, such that the mRV serves as the systemic ventricle and the tricuspid valve (TV) serves as the systemic atrioventircular valve. In physiologic repair, the systemic right ventricle (RV) eventually fails with the time. Because of disappointing results of physiologic repair,2)3)4) the anatomic repair was developed for improvement of long-term results by restoring the left ventricle (LV) and the mitral valve to the systemic circulation, especially in ccTGA patients with mRV failure or TR. Anatomic repair includes atrial switch (Senning/Mustard) operation plus arterial switch (Janene) operation or Rastelli operation.
However, anatomic repair has a high risk of morbidity and mortality due to complexity of the procedure, even in high-volume centers. One-and-a-half modification of anatomic repair using hemi-Mustard procedure can reduce technical demands. With accumulated experience and modification of procedures, the outcome of anatomic repair has improved.5)6)7)8) We have modified the Mustard procedure by adding a bidirectional cavopulmonary shunt (BCPS) in the atrial switch procedure (hemi-Mustard procedure) of anatomic repair in selected patients, as reported previously.9)10)
The aims of this study were to determine the early and late outcomes of anatomic repair of ccTGA and evaluate the effectiveness of hemi-Mustard procedure.
Subjects and Methods
This study was approved by the Institutional Review Board of the Samsung Medical Center, Seoul, Korea, and individual patient consent was waived. Between July 1996 and December 2013, 16 patients with ccTGA underwent anatomic repair at our institution, of which nine were boys and seven were girls. The median age at the time of operation was 3.5 years (range: 0.5-29.7), and the median body weight was 13.3 kg (range: 5.8-54). All patients had ventricular septal defect (VSD). Eleven patients (69%) had left ventricular outflow track obstruction (LVOTO), six (38%) had some degree of pulmonary stenosis (PS), and five (31%) had pulmonary atresia (PA). Six patients (38%) had more than moderate degree of TR. Eight patients (50%) had dextrocardia, and two patients showed situs inversus. Details of each patient's profile, segmental anatomy, pulmonary outflow track obstruction, and TR grade were described in Table 1.
For the atrial switch procedure, the hemi-Mustard procedure was performed in 11 patients, the Senning procedure in four, and the Mustard procedure in one (Fig. 1). To correct the ventriculoarterial discordance, the Rastelli procedure was performed in 11 patients and the arterial switch procedure (Jatene procedure) in five. An aortic homograft or pulmonary homograft was used for the Rastelli procedure. The median size of the conduit was 18 mm (range: 14-27). Six patients with significant TR underwent TV repair with the Kay procedure and/or anteroseptal commissuroplasty.
Surgical technique for the hemi-Mustard procedure combined with the Rastelli procedure
A large piece of pericardium was harvested and fixed with glutaraldehyde solution. A moderate degree of hypothermia and pH-stat strategy were used. Myocardial protection was achieved with multiple intermittent antegrade cold blood cardioplegia.
After opening of the right atrium and inspection of the VSD through the mitral valve, a longitudinal right ventriculotomy incision was made between the stay sutures in a portion devoid of coronary arteries. A baffle was created from the morphologic left ventricle to the aorta with a Dacron patch using multiple interrupted sutures at the inferior margin of the VSD and continuous sutures and anterior and superior margins around the aortic annulus. The atrial septum was removed completely, and the coronary sinus was unroofed. An atrial baffle was made from the inferior vena cava (IVC) to the TV using autologous pericardium or bovine pericardium. After dividing the superior vena cava (SVC) just above the RA-SVC junction, the proximal SVC stump was closed with double-layer sutures. The main pulmonary artery was divided, and the proximal stump was closed with double-layer sutures. Continuity from the right ventricle to the pulmonary artery was established using a homograft conduit 14-27 mm in diameter (small-size bicuspidalized homograft).11) Homograft conduits were placed to the left side of the aorta to avoid compression by the sternum. During the proximal anastomosis, we routinely added a hood of bovine pericardium between the proximal part of the homograft conduit and the RV (Fig. 2). After removal of the aortic cross clamp, the right atriotomy was closed. An anastomosis between the distal SVC and the pulmonary artery was performed in the beating heart. The patient was weaned from cardiopulmonary bypass with careful monitoring of right ventricular pressure. Modified ultrafiltration was performed routinely. The median cardiopulmonary bypass time was 286 minutes (range: 227-531), and the median aortic cross-clamp time was 189 minutes (range: 154-278).
Follow-up
All patients were followed up regularly with echocardiography for a median of 7.7 years (range: 0.8-17.4). Cardiac catheterization was undertaken when more precise hemodynamic or angiographic information was required in patients with symptoms or significant echocardiographic findings.
Statistical analysis
Data were collected retrospectively. Continuous variables are expressed as median and range, and categorical variables were expressed as percentage. Serial data were compared between groups using student's t test. All statistical analyses were performed using IBM SPSS Statistics software for Microsoft (version 22; IBM SPSS, Inc., Armonk, NY, USA). Survival rate and reoperation-free rate analysis was performed using the Kaplan-Meier method.
Results
Before receiving the anatomic repair, five patients without PS or PA required pulmonary artery banding (PAB) to control congestive heart failure and protect the pulmonary artery vascular beds. In patients with ccTGA without PS or PA, PAB has an additional role in the preparation and training of the morphologic left ventricle (mLV). In our series, however, all patients except one had a large VSD. The mLV is already exposed to systemic pressure. The primary purpose of PAB was to protect lungs from pulmonary overflow in most of patients without PS or PA. The one (patient 14) who had a small-to-moderate VSD underwent PAB due to pulmonary overflow mainly caused by atrial shunt, which associated with complete atrioventricular septal defect. The patient had adequate mLV function without additional tightening for mLV training and the pressure gradient at PAB site was 72 mmHg before double-switch operation. Among these PAB patients, one patient underwent a palliative arterial switch operation and 3 months later, underwent an atrial switch operation. Among the patients with PS or PA, two patients had balloon valvuloplasty for the initial palliation because of severe PS. Eight modified Blalock-Taussig shunts were performed in five patients with PA or PS. Two of these patients received a BCPS at 6 months of age because it was difficult to decide whether biventricular repair was possible, and these patients received anatomic repair at 28 and 44 months of age, respectively (Fig. 1).
Early outcomes
There was one in-hospital death (6.5%). A 6-year-old boy (patient 5) underwent anatomic repair using the hemi-Mustard procedure combined with the Rastelli procedure. VSD extension and mitral valve annuloplasty were performed simultaneously. Immediately after the operation, the patient's hemodynamics were stable and extubation was performed 6 hours after the operation. At 10 hours after the operation, the patients experienced a sudden attack of ventricular tachycardia and circulatory collapse, and resuscitation was unsuccessful.
In the 15 survivors, the median ventilator support time was 38 hours (range: 14.3-505), the median stay in the intensive care unit was 5 days (range: 4-35), and the median duration of hospitalization was 32 days (range: 11-64). Postoperative morbidity included prolonged pleural effusion in four patients, transient arrhythmia in four, complete atrioventricular block and pacemaker insertion in three, severe pulmonary edema in two patients who had received a BCPS before the anatomic repair, aspiration pneumonia in two, and pericardial effusion in one patient.
Late outcomes
Among the 15 survivors, there were no late deaths during the follow-up. All patients except one were classified as New York Heart Association (NYHA) functional class I at the last follow-up. The other patient was classified as NYHA class II. Ten patients showed no intra-atrial venous stenosis in an echocardiogram. Five patients showed mild intra-atrial tunnel stenosis in an echocardiogram without hemodynamic significance. One patient showed mild aortic regurgitation, and two patients showed a mild to moderate degree of mitral regurgitation. Three patients showed intermittent atrial tachycardia, and one patient needed permanent pacemaker insertion 1 year after the operation. The TR grade changed after the operation, as shown in Fig. 3. At the last follow-up, all patients exhibited mild or less than mild TR except for one who showed moderate TR.
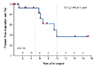
Balloon dilatation for systemic venous pathway obstruction was performed in two patients 12 months and 42 months after the operation. Reoperations were performed in six patients (Table 2). Four patients required a reoperation mainly because of right ventricle to pulmonary artery (RV-PA) conduit stenosis, and two patients required a reoperation mainly because of LVOTO. The median interval between the double-switch operation and the reoperation was 77 months (range: 14-119). Associated residual lesions or recurrent defects were treated simultaneously during the reoperation even though those lesions were hemodynamically insignificant. RV-PA conduit stenosis developed in six patients who had received the bicuspidalized homograft at the time of anatomic repair because of low body weight. Conduit changes were performed with a 18-22 mm-sized Edwards Prima Plus stentless porcine bioprosthesis (Edwards Lifesciences, Irvine, CA, USA) in five patients and with a 21 mm-sized Carpentier-Edwards PERIMOUNT Magna Aortic Heart Valve (Edwards Lifesciences) combined with a 22 mm-sized GORE-TEX Vascular Graft (W. L. Gore & Associates Inc., Flagstaff, AZ, USA) in one patient. Three patients developed LVOTO and underwent VSD extension for relief of LVOTO. Three patients underwent concomitant intra-atrial venous pathway widening because of mild stenosis. One patient required permanent pacemaker implantation because of second-degree atrioventricular block. The freedom from reoperation rate at 5 years was 92.3% (Fig. 4).
Discussion
Anatomic repair in ccTGA has a higher early morbidity and mortality than conventional repair because of the complexity of the procedure. The incidence of ccTGA is low, and it is difficult for the surgeon in a small-volume center to gain sufficient experience to acquire the skills needed to perform the surgery. In our series, even though the early morbidity was high, the mortality and late morbidity rates, except for the conduit changes, were low. The modification of the atrial switch procedure (hemi-Mustard procedure) was likely the main reason for the reduction in the early mortality rate, despite the small volume of cases and little experience in this complex field.
The Mustard atrial switch procedure can be done easily with a generous autologous patch or heterologous pericardial patch. However, the pericardial patch is easily calcified and does not have growth potential, and the long-term results show frequent late stenosis of the caval pathway. A suture line occurs near the sinus node in the Mustard atrial switch procedure, and this increases the risk of sinus nodal dysfunction and risk of late mortality.12) Many centers have reported excellent outcomes of anatomic repair using conventional atrial switch procedures such as the Senning procedure. The Senning procedure has the advantages of avoiding the use of foreign materials and good growth potential, and can be done without postoperative caval obstruction of anatomic features.13)14) Horer et al.15) reported that a reoperation is rarely needed because of baffle stenosis or leaks following the Senning operation.However, the Senning procedure is not easy for inexperienced surgeons or for those in small-volume centers. Most patients with TGA can undergo the arterial switch operation, but the atrial switch procedure is a challenge to learn. A successful Senning procedure needs greater technical skill and more experience. Although some centers recommend the Senning procedure for all types of anatomic features,13) it is difficult to undertake this procedure in patients with ccTGA with situs inversus or situs solitus and dextrocardia, especially for the surgeon in a small-volume center.
To overcome these limitations of the atrial switch procedure, in the modification of the Mustard procedure, an intra-atrial baffle is reconstructed to direct the systemic venous blood flow from the IVC to the mRV through the TV, and the BCPS is added in the hemi-Mustard procedure.16) We prefer the hemi-Mustard procedure as an atrial procedure combined with the Rastelli procedure because of the following advantages. First, compared with the conventional atrial procedure, the hemi-Mustard procedure is technically easy even for the inexperienced surgeon.10)17) It reduces the aortic cross clamp and bypass times, which are the major risk factors for early mortality.18) In a patient with ccTGA with situs inversus or situs solitus and dextrocardia, this procedure is feasible using an approach through the left-sided atrium. Second, the hemi-Mustard procedure reduces the risk of complications of the atrial switch operation such as baffle leak, late venous obstruction, and sinus node dysfunction, which are causes of late morbidity after atrial procedures.17) Third, use of the hemi-Mustard procedure facilitates the Rastelli procedure even in a patient with a small RV. Adding BCPS enables the RV to receive blood only from the IVC, so that even a patient with a relatively small RV can endure the Rastelli procedure. Fourth, TR can be lessened because of the reduced volume load after the hemi-Mustard procedure. Finally, reduced mRV volume load would delay the timing of the RV-PA conduit change.19)20) Malhotra et al.9) reported that only two revisions of the RV-PA conduit were performed among 25 patients who underwent the hemi-Mustard procedure at 11.6 and 12.4 years after the double switch operation during a median follow-up of 4.9 years (range:7 months-16 years). This shows that RV-PA conduit longevity is significantly improved by the hemi-Mustard procedure.
Because of high early mortality and morbidity, we adopted hemi-Mustard modification of anatomic repair since 1999. Increased pulmonary vascular resistance is a well-known contraindication of BCPS. One patient (patient 15) who had significantly high pulmonary artery pressure required Senning plus Jatene operation. With experience, we performed additional two Senning plus Jatene operations. The one (patient 12) needed repair for severe TR during early infancy. The other (patient 14) was suitable for making the systemic venous pathway to mRV because of associated primum atrial septal defect. The hemi-Mustard procedure has several advantages in patients who require Rastelli procedure. By reducing the volume across the right ventricular-pulmonary artery conduit, the durability of the conduit can be prolonged. The mRV function can usually be reduced during the Rastelli procedure. The hemi-Mustard procedure can reduce the volume load on the impaired mRV. In summary, we prefer the hemi-Mustard modification except in patients with high pulmonary vascular resistance and in early infants. We choose the hemi-Mustard procedure preferentially in patients who underwent Rastelli procedure. However, with increasing experience, and considering the long-term functional outcomes compared to biventricular repair, we aim to perform the Senning operation instead of the hemi-Mustard operation in select patients with adequate mRV function, no TV dysplasia, and suitable anatomy (such as no positional anomalies).
In patients with no LVOTO receiving the arterial switch procedure, the Senning procedure is preferred because it avoids the use of foreign materials and can anticipate growth. The recently introduced use of autologous pericardium or bovine pericardium makes the procedure easier.
The size of the VSD is a critical point in the anatomic correction combined with the Rastelli procedure to repair ccTGA. When the size of VSD is not suitable for making an intraventricular tunnel from the mLV to the aorta, a VSD extension is inevitable, but can cause conduction disturbance or coronary artery injury in the septum. An insufficient VSD extension would result in residual or late LVOTO. This becomes more difficult because there is no guide for anticipating the possibility of a future LVOTO after the Rastelli procedure. Late LVOTO because of the small size of the VSD occurred during follow-up. We also had to perform VSD extension in two patients after the correction. The mechanism responsible for the late LVOTO is unclear; however, one possible explanation is that, at the time of first corrective surgery, we underestimated the size of the VSD and omitted an additional procedure to extend the VSD. Another possible explanation is that, in patients with PA, the size of the VSD is equal to that of the aortic valve to accommodate all of the systemic blood flow. By contrast, in patients with PS, the systemic venous blood flow is separated into two outflows, and the size of the VSD is restricted because some of the systemic venous blood flow goes through the VSD. If these explanations are correct, intraventricular rerouting with the Damus-Kaye-Stansel procedure could be used to make a non-obstructive systemic ventricular outflow tract without VSD enlargement, regardless of whether the size of the VSD is restrictive.13)
Sometimes, when using a procedure for VSD extension to correct a restricted VSD, a surgical block can develop and requires insertion of a permanent pacemaker. The exact location of the conduction system in this anatomic group has not been identified precisely.21) During the septal extension of the VSD, injury of the septal penetrating branch is another factor that could affect systemic ventricular function.22) Damage to the septal penetrating branch can result in severe ventricular dysfunction and death.
Another consideration is the inevitable conduit change after the Rastelli procedure, especially in young patients during the initial procedure. The causes of conduit failure include functional homograft failure, somatic outgrowth over small-sized, and technical failure. One advantage of the hemi-Mustard-Rastelli procedure is a delay in the timing of the RV-PA conduit change.12)13) In our series, four patients required a reoperation mainly because of RV-PA conduit stenosis. The median age of these patients at the time of the first operation was of 2.2 years (range: 1.4-61.0), and the median interval between the first operation and the reoperation was 7.7 years (range: 5.8-9.9). Because of the young age of the patients at the time of the first operation, we used a small-sized bicuspidalized homograft,10) and conduct stenosis was unavoidable considering the increase in body weight and size after this age.
One cannot always decide which strategy (Fontan procedure or anatomic repair) is optimal for every patient. Anatomic repair has a high surgical risk because of the small size of the mRV, the complex anatomy, and young age of patients. In these situations, one strategy is to perform a BCPS in an infant and delay the decision-making until the time of the Fontan procedure.17) We applied this strategy in two patients, and the anatomic repair was successful at 2 years of age in both patients. An interesting finding was that, after anatomic repair, both patients exhibited postoperative pulmonary edema. One patient recovered with the aid of a high-frequency ventilator and the other patient recovered with the support of extracorporeal membrane oxygenation. We cannot speculate on the exact reason for the pulmonary edema. One possible explanation is that it occurred because of the relatively high pressure and volume load applied to the chronically low pressure- and low volume-loaded lung system.
Development of TR in ccTGA is part of the natural history of this anatomy because of the high-pressure load and dysfunction of the right ventricle. This can be improved by PAB for LV preparation23)24) or anatomic repair,25) because these procedures cause changes in the geometry of the right and left ventricles, and the TV is faced with the situation of a low-pressure chamber. However, some types of TV associated with ccTGA have dysplastic features such as Ebsteinoid dysplasia, which needs valvuloplasty during the anatomic repair to reduce TR.7) As in the techniques used for the tricuspid valvuloplasty, one may consider commissural closure, suture annuloplasty, annulus plication, or cleft repair. These techniques are not difficult and do not require much time. We performed tricuspid valvuloplasty in six patients who had TR of more than a mild to moderate degree. All of the patients except one had an improved regurgitation grade at the last follow-up. Simple repair techniques were sufficient to avoid significant TR.7) Although the Fontan operation is another way to deal with the ccTGA, the best outcome was from Fontan operation for non-ccTGA. Data regarding Fontan outcome in ccTGA compared to other repairs is limited to date. Shin'oka et al.26) failed to demonstrate the superiority of anatomic over classical repair unless patients had significant TR preoperatively. However, because there were no longer-term results, we were unable to confirm the superiority of approaches.
The major limitations of this study include its retrospective design and small number of patients. In addition, the postoperative echocardiographic assessment was only semiquantitative. The long-term results of one and one-half ventricle repair are not well documented, and long-term observation and analysis are needed.
Anatomic repair can be performed with low risk of mortality even in a small-volume center. When applied to a select group of patients, the hemi-Mustard strategy can be one solution to reduce the early mortality and morbidity, and the risk of long-term complications such as venous pathway stenosis, sinus node dysfunction, and conduit change. The hemi-Mustard strategy might also have benefits such as preserving cardiac function and preventing TR, but long-term follow-up is needed to confirm this conclusion.





 XML Download
XML Download