

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cellular loss of cardiomyocytes in myocardium mostly through myocardial ischemia or infarction, so-called ischemic cardiomyopathy, causes functional limitation of the remaining heart and finally contributes to heart failure. Ischemic cardiomyopathy caused more than seven million annual deaths worldwide, and patients suffering from this condition lead a very deprived life.1) Although many therapeutic options including revascularization, medication, and even cardiac resynchronization have been adopted for the treatment of patients with ischemic cardiomyopathy, current treatment options are still far from the myocardial regeneration. Therefore, strategies including cell therapy and specific implantation of cells which have potential to induce myocardial regeneration, have been of particular interest. Recently, the international federation for adipose therapeutics and science stated that adipose-tissue derived stem cells (ADSCs) could be one of the ideal biological cellular resources for regenerative medicine applications.2)
During the last several decades, ADSCs have been studied as potential cellular resources for tissue regeneration. ADSCs mean ‘stem cells’ derived from adipose tissue. ADSCs have been known to have potential to differentiate in vitro into adipogenic, osteogenic, chondrogenic, and myogenic cells as well as endothelial cells.3)4)5)6)7)8)9)10) Many studies have identified ADSCs as heterogeneous mesenchymal cells (except adipocytes) derived from adipose tissue.11) ‘Stromal vascular fraction’ have also been used to indicate ADSC. Previous studies showed some discrepancies probably due to different isolation procedures and culturing methods as well as the absence of the standard purifying methods for homogenous cell population. Some cell surface markers were reported to vary at different passage numbers.12) Thus, each ADSC population might need to be assessed for their suitability before clinical applications are ensured. Many recent studies have suggested therapeutic potential of ADSC as cell therapy for many different diseases including myocardial infarction. In this review, we focused on clinical application of ADSC for myocardial regeneration.
What is Adipose Tissue Derived Stem Cell?
In the 1960s, Rodbell13) firstly found the method to isolate cells from rat adipose tissue. In the 2000s, Zuk et al.4) modified and developed ADSC isolation method from human adipose tissue and suggested that ADSC as a promising source for adult multipotent stem cells.14) Recently, Nicoletti et al.15) also developed a new ADSC isolation protocol using enzymatic digestion. D'Andrea et al.16) reported a successful long-term (4 months) and large-scaled ADSC culture. However, it is still necessary to establish a standardized ADSC isolation protocol, which can warrant homogenous ADSC population and reproducible results for clinical application. Although ADSCs have tendency to differentiate into adipocytes,17) they have potential to differentiate into other lineage cells including osteoblasts,18)19) chondrocytes,20) endothelial cells,21)22) and myogenic cells23)
in vitro, which are comparable to bone marrow derived mesenchymal stem cells (BMSCs).21)24) Similar to BMSCs, ADSCs secrete many different kinds of growth factors and cytokines which could contribute in stimulating angiogenesis as well as myocardial regeneration.25)
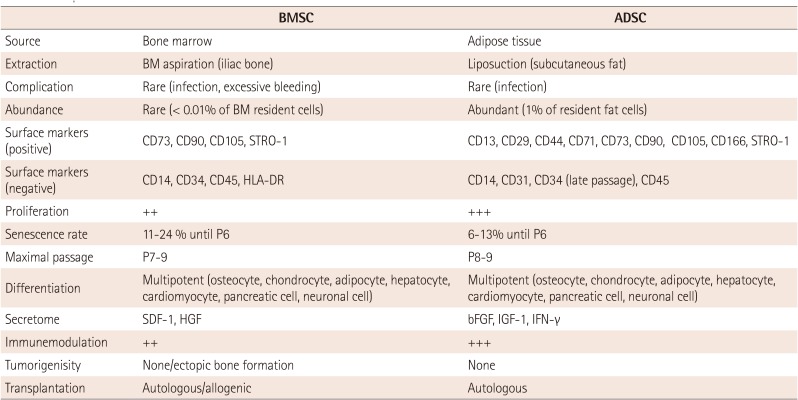
In the perspectives of cell therapy, ADSCs have several advantages. ADSC can be easily isolated from the adipose tissues which are obtained in relatively large amounts by liposuction. Its efficiency was known to be up to 100 times as compared to BMSCs.26)27)28) Thus, immediate autologous implantation of ADSCs without further in vitro cell culture could be feasible. Detailed comparisons of cellular characteristics between ADSC and BMSC are summarized in Table 1.29)30)31)32)
Mechanisms for Myocardial Regeneration
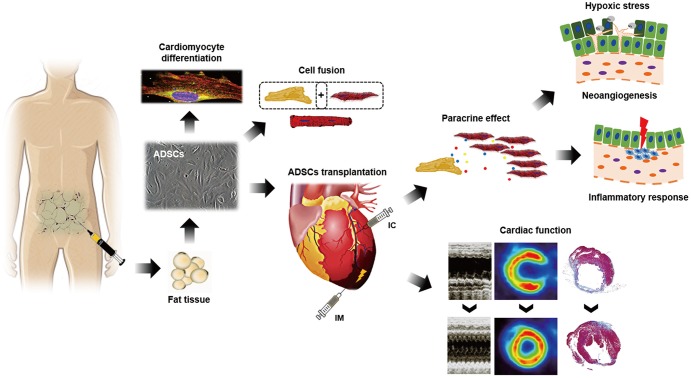
The mechanisms underlying the effects of ADSCs for myocardial regeneration have not been fully elucidated (Fig. 1). Previously, ADSCs have been reported to have direct differentiation potential into cardiomyocytes in vitro.24) Bai et al.33) demonstrated human ADSC-derived cardiomyocytes expressing connexin 43 and troponin I in mouse acute myocardial infarction (AMI) model, which suggested in vivo cardiomyocyte differentiation of ADSC through fusion-independent mechanism. However, most of the previous in vivo studies on ADSC implantation suggested that only a small fraction of implanted ADSCs contributed into the possible in vivo cardiomyocyte differentiation.34)35) Cell-fusion and mitochondria transfer might also contribute to ADSC-derived cardiomyocytes.36) On the other hand, Yang et al.37) failed to detect ADSC-derived cardiomyocytes although ADSC-derived vascular cells were measured up to 9% of the enhanced angiogenesis. Other study also reported no specific findings of transdifferentiation of ADSC.38)
Predominant suggested mechanisms of ADSCs for myocardial regeneration were their paracrine effects.39)40) ADSCs have been known for secreting many different kinds of proangiogenic, anti-apoptotic and immunomodulatory cytokines and growth factors in the implanted myocardium after ischemic injury.37)41) Productions of various paracrine factors are thought to be enhanced even under hypoxic stress.42) These factors rescue the endangered cardiomyocytes, promote neoangiogenesis and prevent exaggeration of inflammatory response. Finally, ADSCs could reduce scar formation and prevent the adverse cardiac remodeling after ischemic injury.41) In addition, ADSCs have been reported to promote recruitment of other progenitor and stem cells. Kondo et al.43) demonstrated SDF-1 expression in mouse ADSC, and reported that implantation of ADSC into the ischemic hindlimb increased recruitment of circulating endothelial progenitor cells through SDF-1 dependent mechanism.
There have been several studies on comparative analysis between ADSC and other cellular resources. When compared with BMSCs, ADSCs showed similar proangiogenic and immunomodulatory potential. Hao et al.44) demonstrated similar recovery capacity of limb perfusion between ADSCs and BMSCs in a rabbit hindlimb ischemic model. Both cell types also similarly suppressed lymphocyte proliferation and activation elicited by mitogen.45) Recently, several studies have reported that human ADSCs revealed higher capacity to reduce the infarct area in rat AMI models as compared to BMSCs.46)47) Rasmussen et al.46) reported that ADSC implantation showed a superior improvement in left ventricular (LV) systolic function as compared to BMSC implantation. Paul et al.47) also demonstrated superior improvement in cardiac function and less scar formation, which were driven by the immunomodulatory effect of implanted ADSCs. Thus, it is proposed that the unique immune tolerance property of ADSC in addition to its angiogenic property could be the important cellular mechanism for tissue regeneration in allogenic or transgenic transplantation models.
Implantation Cell Number
Because most of the ADSCs were rapidly washed out or phagocytosed after implantation, it has been hypothesized that larger number of ADSC implantation might induce more engraftment of the residual ADSCs, which could enhance their therapeutic potential in vivo. However, there have been very few studies regarding neither an optimal implantation dose of ADSCs nor their possible dose-response relationship.48) Naaijkens et al.49) extensively reviewed previous studies regarding the implantation cell number and its functional capacity. In small animal models, 5/13 (38%) studies involving less than 1 million of implanted ADSCs showed a significant infarct size reduction as compared to 12/15 (80%) studies involving more than 1 million of implanted ADSCs. For LV systolic function, 10/17 (59%) studies involving less than 1 million of implanted ADSC showed a significant increase in left ventricular ejection fraction (LVEF) as compared to 12/15 (80%) studies with more than 1 million ADSC implantations. In contrast, studies on the immune-deficient animal model showed less pronounced dose dependencies with respect to increase in blood vessels; whereas in studies involving immune-deficient animal model, significant reduction in infarct size was found in 3 out of 4 (75%) studies using less than 1 million of implanted ADSC as compared with 5 out of 5 (100%) studies using more than 1 million ADSC. The researchers also compared the efficacy of less than 50 million or more ADSC implantation with studies conducted in large animal models by implanting more ADSCs. Similar to the small animal models, studies using larger number of ADSC implantation showed positive results more frequently. Thus, it has been suggested that larger number of ADSC implantation could be beneficial in reducing infarct size and in inducing myocardial recovery. Considering the rapid cellular wash-out in vivo, the optimal delivery method, which is as important as the delivered total ADSC number, to enhance the in vivo engraftment of the implanted ADSC should also be explored.
Delivery Methods
The delivery method of stem cell implantation is an important determinant for effective cell therapy. Until now, three main different delivery routes of intramyocardial, intravenous, and intracoronary injections have been widely used. Compared to intramyocardial and intracoronary injections, intravenous injection has been contemplated to deliver smaller number of stem cells into the injured myocardium due to the pulmonary first pass effect.50) Nonetheless, intravenous injection of ADSC showed beneficial effects on reducing infarct size and even enhancing cardiac function and blood vessel formation in several animal studies.51)52) Therefore, several human clinical trials have adopted intravenous injection with respect to advantageous and less invasive procedure.
Intracoronary administration of ADSCs has also been considered for its selective delivery into the target myocardium. Firstly, intracoronary administration of ADSC showed similar improvement in myocardial perfusion and LV systolic function as compared to BMSC in porcine AMI model.53) In six large animal studies of ADSC implantation reviewed by Naaijkens et al.,49) 3/4 (75%) studies involving intramuscular injection decreased myocardial infarct size significantly as compared to 1/3 (33%) studies involving intracoronary injection. For LV systolic function, 2/4 (50%) studies involving intramuscular injection increased LVEF significantly as compared to 2/3 (67%) studies relating intracoronary injection. For angiogenesis, 2/4 (50%) studies involving intramuscular injection increased blood vessels significantly as compared to 3/3 (100%) studies dealing with intracoronary injection.54)55)56)57)58) Although there are limited numbers of studies, previous studies suggested that intracoronary injection could be comparable to intramuscular injection for myocardial recovery. Notably, Hong et al.59) compared the cell retention rates of ADSCs between intracoronary and retrograde coronary venous delivery methods in porcine AMI model. Intracoronary injections showed the potential risk of coronary microcirculatory obstructions and early redistribution within 24 hours of injection of ADSCs into pulmonary circulation.
Numerous studies employing small animals have adopted intramyocardial injections. However, intramyocardial injections still show the limitation of cellular engraftment in the infarcted myocardium. Many attempts have been proposed to overcome this obstacle like, a few novel hydrogels have been introduced as potential delivery methods for ADSCs. Wang et al.60) developed chitosan-based hydrogel and implantation of ADSCs mixed with chitosan hydrogel significantly improved LV systolic function as well as cellular engraftment. Notably, chitosan-induced cardiomyocyte differentiation of ADSC both in vitro and in vivo has been demonstrated in their study. Similarly, ADSCs embedded platelet-rich fibrin scaffold revealed further improvement in LV systolic function and LV remodeling as compared to direct implantation of ADSC in rat AMI model.61) Recently, cell sheet technology was introduced to improve cell engraftment after stem cell implantation. Ishii et al.62) developed multilayered ADSC sheet by magnetite tissue engineering technology and transplanted multilayered ADSC sheet epicardially in mouse AMI model. ADSC sheet significantly improved LV systolic function as well as neovascularization in infarct area. Yeh et al.63) developed vascular endothelial growth factor-overexpressing ADSC sheets and applied them in rabbit AMI model with demonstrable near normalized functional recovery of the infarcted myocardium by the epicardial implantation of such sheets. Moreover, application of ADSC sheet improved LV systolic function in a porcine chronic myocardial infarction model.64)
Human Trials
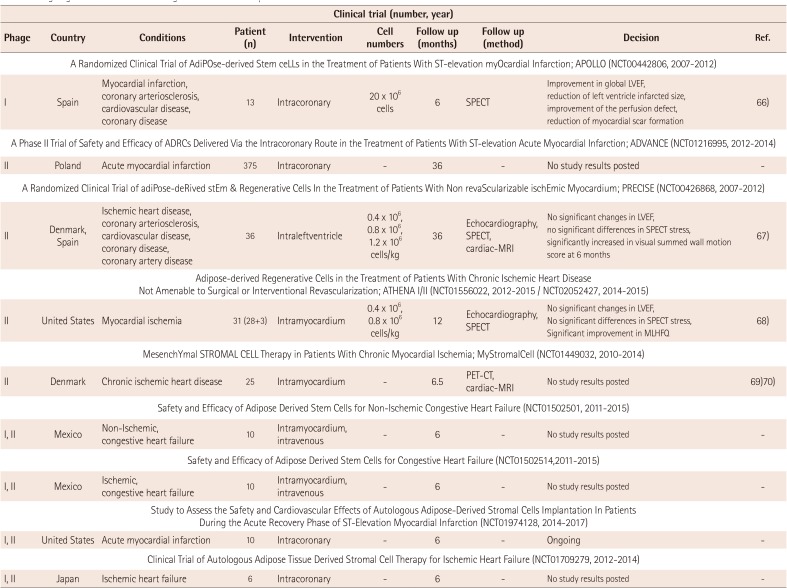
To date, there have been several human clinical trials of ADSCs for ischemic heart diseases (Table 2). 65) Houtgraaf et al.66) firstly reported the safety and efficacy of ADSC in patients with AMI (APOLLO trial; randomized, double-blind placebo-controlled, phase I/IIa study). The study involved infusion of 20 million ADSCs, freshly isolated by liposuction, via infarct related coronary artery into the injured myocardium within 24 hours after primary percutaneous coronary intervention. At 6 months follow-up, cardiac magnetic resonance imaging (MRI) and MIBI-SPECT showed a trend towards the improved LVEF as compared to the placebo group, accompanied by a significant reduction in the perfusion defect and infarct size. Moreover, there were no adverse events during the procedure. The ADVANCE trial, another clinical trial regarding intracoronary injection of ADSCs for patients with AMI, was performed and now final results are awaited.
Perin et al.67) reported the PRECISE trial which was the randomized, placebo-controlled, double-blind trial of transendocardial injection of ADSCs in patients with refractory ischemic cardiomyopathy. Transendocardial injection of ADSCs preserved LV mass and the regional wall motion determined by cardiac MRI and improved myocardial perfusion determined by single-photon emission CT as well as exercise capacity. Other ongoing human clinical trials of ADSCs for ischemic heart diseases include the ATHENA I and II trial (Cytori Therapeutics; intramyocardial injection),68) the MyStromalCell tria (Rigshospitalet, Denmark; allogenic ADSC; intramyocardial injection),69)70) the NCT01502501 trial (Ageless Regenerative Institute; intramyocardial/intravenous injection), the NCT01502514 trial (Ageless Regenerative Institute; intramyocardial/intravenous injection), the NCT01974128 trial (Ageless Regenerative Institute; intramyocardial/intravenous injection), and the NCT01709279 trial (Kanazawa University; intracoronary injection).
Conclusion
During the last several decades, cell therapy using adult stem cells has emerged as a future therapeutics especially for ischemic heart diseases. Among them, ADSCs are very attractive cellular resource for their relatively easy accessibility in large amount, potent differentiation properties, and powerful paracrine effects. Previous animal studies have demonstrated promising results of ADSC implantation for myocardial recovery in ischemic heart diseases, and recent studies focused on the improvement of its efficacy by enhancing their therapeutic potential through genetic modification and cellular priming, in addition to development of novel delivery methods using hydrogels and cell sheet technology. Human clinical trials also support the safety and therapeutic efficacy of ADSCs for myocardial regeneration. Many clinical trials are still ongoing to step forward in clinical research and application.
 XML Download
XML Download