

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Carotid ultrasound is one of the several imaging modalities that allow non-invasive assessment of vascular anatomy and function.1)2) Use of this technique allows measurement of a variety of parameters including intima-media thickness (IMT), arterial diameter, the presence of plaque, blood flow and velocity measurements. The typical B-mode image of the arterial wall is defined as the double line pattern, in which the inner line is generated by the intima surface, and this imaging approach is a useful and safe tool for the measurement of IMT.3) In addition, the consensus statement from the American Society of Echocardiography has simplified carotid IMT and plaque assessment methodology.4)
Carotid IMT and presence of plaque have been shown to predict cardiovascular events in multiple large studies.5)6)7)8) Also, in low-risk subjects, initial screening by IMT and plaque assessment is likely to provide useful information for the detection of subclinical atherosclerosis.9) Furthermore, common carotid blood flow (CBF) velocity was independently associated with future cardiovascular disease (CVD) using color duplex ultrasound and Doppler spectral analysis.10) In clinical practice, evaluation of the carotid artery by ultrasonography is a very useful, simple, and safe method to indirectly detect and prevent CVD.
However, in 2013, American College of Cardiology/American Heart Association (ACC/AHA) guidelines for cardiovascular risk assessment designated that the carotid IMT as class III evidence level was not recommended for use in clinical practice as a routine measurement of risk assessment for a first atherosclerotic cardiovascular disease (ASCVD) event.11) After the announcement of this guideline, Naqvi et al.12) reported that the controversy surrounding the usefulness of carotid IMT measurement in risk stratification appears to result from the lack of a uniform methodology in carotid IMT studies.
This article reviews the studies performed after the announcement of this guideline and which evaluated carotid IMT for ASCVD risk prediction and risk estimation in a specific condition. In addition, this article discusses the value of common carotid IMT (CCA-IMT) and plaque parameters in CVD risk assessment and prediction. The article summarizes the studies using hemodynamic parameters of the carotid artery in CVD risk association or prediction and also discusses the separate measurement of carotid IMT and its usefulness and limitations in clinical practice.
Carotid intima-media thickness measurement
Carotid IMT is used to measure the distance between the luminal border of the intima and the outer border of the media of the carotid artery far wall, which is represented as a double-line pattern on a B-mode ultrasound image (Fig. 1).3)4) The carotid artery includes four segments: common carotid artery (CCA), bifurcation (bulb), external carotid artery and internal carotid artery (ICA). The IMT can be measured in the CCA, bulb, and ICA.13) Among the limitations frequently cited in measurement of carotid IMT is the difficulty in appropriately imaging all carotid artery segments, especially the ICA-IMT.
In the Atherosclerosis Risk in Communities (ARIC) study, 91.4% of the CCA-IMT segments could be adequately imaged compared with 77.3% of bulb IMT segments and 48.6% of ICA-IMT segments.5) Similarly, in the Rotterdam study, carotid IMT measurements were possible in 96% of the CCA-IMT segments compared with 64% of bulb-IMT segments and 31% of ICA-IMT segments.14)
Considering accuracy and best reproducibility, CCA far wall IMT measurement was validated as representing the true thickness of the vessel wall.13) The development of automated edge detection programs for use instead of manual measurements has increased the speed and reduced the variability of measurements.15)
Separate measurements and clinical implications
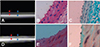
Carotid IMT is the sum of the intima thickness (IT) and the media thickness (MT) (Fig. 1). In an animal study, the carotid high-echogenic intimal thickening (HEIT) examined using a 40 MHz correlates closely with the histological IT (Fig. 2).16) Separate measurements of the individual intima and media layers in carotid arteries can be examined using high-resolution B-mode ultrasound.17) Remodeling of the thickness of the intima and media layers is a distinct process that exhibits independent changes in different types of arteries with advancing age and throughout the development of atherosclerosis.18) Early vascular changes caused by atherosclerosis occur primarily in the IT.17) Thus, the IT can be a useful parameter for early detection, prediction of progression and evaluation of atherosclerosis.19) Increased IMT in hypertensive patients is caused by increased MT and is compatible with medial hypertrophy seen in hypertension.20) Therefore, separate measurements are useful for assessing the effects of different atherosclerotic risk factors on the arterial wall.21)
However, the theoretical axial resolution of a 7 MHz transducer is approximately 0.3 mm, and the high-frequency (about 11-15 MHz transducer) ultrasound pixel resolution is approximately 0.1 to 0.2 mm.22) Therefore, if the IMT complex is thinner than 0.3 mm, the leading edges of the two echo interfaces from far wall intima and adventitia respectively cannot be separated, and measurement of the intima–media complex is not possible using a 7 MHz transducer.22) Furthermore, the mean IT is approximately 0.2 mm and it can be intermittently or inadequately measured even by using a high-frequency transducer. This limitation should be the focus of attention in future studies. In addition, the annual change of carotid IMT value is approximately 0.01 to 0.04 mm per year in the general population23) and patients with disease;24) this is lower than the current resolution of ultrasound. Therefore, it is impossible to analyze carotid IMT change over a short period.
Carotid intima-media thickness and carotid plaque assessment for cardiovascular risk prediction
A meta-analysis of 14 population-based studies that evaluated CCA-IMT alone and excluded CCA, bulb IMT and plaque showed that the addition of CCA-IMT measurement to the Framingham Risk Score was associated with small improvement in 10-year risk prediction of first-time myocardial infarction or stroke, but this improvement is unlikely to be of clinical importance.6)25) However, CCA-IMT including the carotid bulb and ICA-IMT were found to be better predictors of both cardiac risk and stroke risk.26) Carotid plaque appears to be a more powerful predictor of CV risk than carotid IMT alone.27) In summary, many previous studies have revealed discrepancies in the comprehensiveness with which carotid IMT was assessed with regard to the number of carotid segments evaluated (CCA, ICA, or the carotid bulb), the type of measurements (mean or maximum of single measurements, mean of the mean, or mean of the maximum for multiple measurements), whether plaques were included in the IMT measurement, use of adjusted or unadjusted models, risk association versus risk prediction, and arbitrary cutoff points for CIMT and plaque to predict risk.12)
After the announcement of the 2013 ACC/AHA guidelines for CV risk assessment,11) the ARIC study reported that coronary heart disease (CHD) risk prediction can be improved by adding all carotid artery segments (A-CIMT) including the presence of plaque or CCA-IMT and plaque information to traditional risk factors (TRF) compared with CCA-IMT alone. Furthermore, because measurement of CCA-IMT is easier and more reliable than A-CIMT, evaluating the carotid artery for plaque presence and measuring CCA-IMT provide a good parameter for CHD risk prediction.28)
In a recent guideline, the carotid IMT was not recommended for use in clinical practice as a routine measurement of risk assessment for a first ASCVD event. Thus, it is unclear when carotid IMT should be measured in clinical practice. In a recent study, carotid plaque was found to be more useful as an additive predictive factor for primary prevention of ASCVD than CCA-IMT alone in asymptomatic high risk patients.29) CCA-IMT and carotid plaque were useful prognostic parameters to predict long-term future CV events in patients with well-treated ST elevation myocardial infarction (MI). The value of CCA-IMT measurement in predicting CV events seems to be of clinical importance beyond the TRF in this relatively low-risk population with acute MI.30) In patients with one or more TRF, carotid plaque is more useful as an additive predictive factor for primary and secondary prevention of ASCVD than is CCA-IMT alone.31)
In a recent study with a small sample size, no significant differences in clinical outcomes from CV events, including death, MI, and stroke were observed between the highest and lowest CCA-IMT values based on the inter-quartile range in the younger subjects (males <45 years and female <55 years) with hypertension.32) Another study reported similar results, showing that, within a relatively young Iranian population of individuals without a history of CV event, thicker carotid IMT did not associate with several modifiable CV risk factors.33)
In the elderly hypertensive population aged at least 60 years, only calcified carotid plaques (except for mean A-CIMT) predicted mortality and cardiovascular outcomes above other traditional CVD risk factors such as age, sex, and hypertensive status.34)
The evaluation of carotid plaque
Carotid plaque is identified as an echoic focal projection, or as the presence of focal wall thickening that is at least 50% greater than that of the surrounding vessel wall or as a focal region with carotid IMT greater than 1.5 mm that protrudes into the lumen and is distinct from the adjacent boundary.4) Other definitions for plaque identification include shadowing in wall texture, roughness, and inconsistency in the visualization of structural boundaries together with bright echogenicity.35) Many previous studies have reported different approaches to the analysis and assessment of plaques, such as recording the absence or presence of plaque,36) the size or burden of plaque (mild, moderate, or severe),37) number of visible plaques (no, single, or multiple)38) and composition or tissue characterization (echolucent, or calcified) (Fig. 3).35)39) However, reliable characterization of plaque tissue content and features suggestive of plaque instability (ulceration, thin fibrous cap) using standard carotid ultrasound techniques is not yet possible. In addition, there is a need for a developing a molecular imaging method that is capable of identifying the echolucent or calcified plaque on carotid ultrasound.
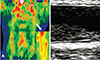
Some studies have attempted to analyze the tissue properties of plaque with ultrasound techniques using different imaging modalities. Using positron emission tomography-computerized tomography, an echolucent plaque has greater F-18 FDG uptake than calcified plaque or no plaque, which seems to imply a high inflammatory state (Fig. 4).40) Calcified regions of the carotid plaque were characterized as white radiodense areas by spiral CT imaging, in contrast to the remaining non-calcified regions of the plaque and lumen.41) Using high-resolution MRI, 71% of the carotid plaques contain a lipid core, which might provide evidence supporting more aggressive cholesterol-lowering therapy.42)
With recent developments in technology, it has become possible to analyze the ultrasound characteristics of complex plaques. Computer-assisted pixel distribution analysis of duplex ultrasound scan images accurately quantified intraplaque hemorrhage, fibromuscular tissue, calcium, and lipid.43) In addition, the emergence of 3-dimensional (3D) ultrasound allows more accurate quantification of plaque volume or area. Plaque areas from all cross-sectional images in the entire image sequence were summed as the plaque burden.44) Therefore, not only the presence or absence of plaques, but also the characteristics of plaques or plaque burden can be evaluated with regard to prognosis of CV events31) and its implications for CV risk.45)
Carotid intima-media thickness and biomarkers of cardiovascular disease
Biomarkers are a convenient method to detect high-risk individuals, to diagnose disease conditions promptly and accurately, and to effectively evaluate the prognosis and treatment outcomes of patients with disease. The role of carotid IMT as a structural marker of the artery and as a biomarker for identifying high-risk patients has been investigated.46) According to the 2013 ACC/AHA guideline, if a risk-based treatment decision is vague after quantitative TRF assessment, evaluation of one or more of the following factors may be considered to make informed treatment decisions: family history, hs-CRP, coronary artery calcium score (CACS), or ankle-brachial index (ABI).11) Assessment of CACS, which is similar in form to a structural biomarker of the artery, is useful for diagnosis and as a surrogate marker of ASCVD compared with CCA-IMT or plaque.31) Carotid plaque and increased carotid IMT are associated with the presence and degree of coronary calcification and disease.47) ABI is a functional biomarker of the artery. In one retrospective study, patients with greater mean CCA-IMT (≥0.9 mm) or lower ABI (<0.9) had significantly higher complexity and presence of CAD. Also, the combination of CCA-IMT and ABI provides additive information for predicting the severity and presence of CAD.48) In another study, the hs-CRP level, which is a serological biomarker of the artery, and carotid plaque characteristics were found to correlate closely with the severity of CAD.49)
Carotid hemodynamic parameters
Carotid ultrasound is widely used to measure hemodynamic parameters such as peak-systolic velocity (PSV), end-diastolic velocity (EDV), and resistive index (RI), calculated as (PSV-EDV)/PSV (Fig. 5).
In a case-control study, stroke patients in an acute as well as a chronic stable phase appeared to have lower CBF velocity and volume and higher RI than non-stroke patients, independent of carotid atherosclerosis.50) In a Taiwanese population at low risk for atherosclerosis, CCA-IMT and EDV could jointly predict the risk of future ischemic stroke events, and EDV value was more strongly associated with ischemic stroke than was CCA-IMT.51) In addition, in a prospective study, carotid flow velocity (CFV) was significantly associated with the development of CVD during a median follow-up time of 12.8 years. CBF velocity, particularly EDV, also improved the risk prediction of CVD.10) In a total of 1,119 Korean patients without CHD or stroke, among the carotid Doppler indices, higher RI, and lower CCA-PSV and CCA-EDV, but not ICA Doppler indices, were related to future CV events.52) Therefore, CFV represents a subclinical atherosclerosis index and it should be included in the assessment of CVD risk.
Future direction
Measurement of CCA-IMT and plaque detection using ultrasound imaging can be easily, simply, safely, and reproducibly accomplished in the outpatient setting as a noninvasive screening method for CV risk assessment. Considerable technical developments are needed to evaluate the characteristics or burden of plaque and to identify plaque reproducibility. Also, abnormal cutoff values for CCA-IMT, plaque presence, and size or volume, adjusted for age, race, and sex remain to be defined. In addition, the reproducibility, abnormal cutoff value, and the role of carotid hemodynamic parameters must be defined in large multicenter studies.
Conclusion
The controversial circumstances in which carotid ultrasound examination is performed raise questions about the usefulness of carotid IMT measurement in risk stratification. The usefulness of carotid IMT measurement in clinical practice remains uncertain. Measurements of carotid IMT at the carotid bulb and at the ICA are more useful than that of CCA-IMT, both for risk classification and risk prediction. However, in view of the accuracy and best reproducibility, CCA-IMT measurement was validated as best representing the thickness of the vessel wall. Future developments in ultrasound technology will focus on separate measurements of the carotid artery to evaluate the effects of different atherosclerotic risk factors on the arterial wall. We posit that separate measurement will play an important role in the evaluation of subclinical atherosclerosis and remodeling of the arterial wall according to a variety of risk factors, such as metabolic syndrome. Assessment of plaque burden or size is a better method of determining atherosclerosis and CV risk than is a simple assessment of the presence or absence of plaques. In addition, plaques that appear echolucent or soft on B-mode ultrasound are lipid rich, whereas echogenic plaques have a higher content of dense fibrous tissue and calcification. The characteristics of an echolucent or soft plaque might provide evidence for more aggressive therapy, although further study is needed to verify this. Combined CCA-IMT and plaque assessment, including plaque tissue characterization and plaque burden, using 3D ultrasound appears to be better than either measurement alone for the assessment and prediction of ASCVD risk. Also, further study is needed to determine the change or remodeling of CCA-IMT and plaque after therapy or intervention. In addition, although carotid hemodynamic parameters are useful tools for risk classification and risk prediction in clinical practice, additional clinical research is needed. Furthermore, plaque progression and regression assessed by 3D ultrasound may be a powerful method to assess the effect of therapy. Groups developing future guidelines should consider the roles of plaque presence and burden and hemodynamic parameters in additional risk stratification beyond carotid IMT.



 XML Download
XML Download