

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Superior vena cava (SVC) drains blood from the head and upper extremities to the heart. When the blood flow becomes limited by extraluminal compression or intraluminal obstruction, SVC syndrome may occur. As SVC obstruction progresses, the blood pressure in the venous system increases and the collateral vessels dilate. The severity of symptoms is related to the speed and degree of SVC narrowing.1)
Bilateral absence of SVC is a rarely reported etiology of SVC syndrome, and it is often found with other congenital cardiac anomalies and/or conduction abnormalities.2) Herein, we report a case of a patient with complete absence of SVC, but without any sign of SVC syndrome and electrical disturbance.
Case
A 27 year-old man was referred to our hospital for evaluation of chronic cough. He was previously healthy, and his only symptom was a one-year history of cough. He denied any neurologic, respiratory and cardiovascular symptoms. He was a current smoker, with 2.5 pack-year smoking history. His vital signs were normal and physical examination was unremarkable; there was no facial and upper extremity swelling, and the lung and heart sounds were normal. He also denied any family history of congenital anomaly of the cardiovascular system. No previous medical illnesses were reported, or any history of pediatric malignancy, central venous catheterization, or chronic infection.
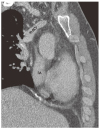
In his initial visit to the hospital, he underwent a chest X-ray and non-contrast computed tomography (CT) scan; was no significant abnormality was seen in the lung parenchyma. Tortuous collateral vascular structure in the anterior mediastinum suggested the possibility of SVC obstruction, but the etiology of the SVC obstruction was unclear in these images. He later underwent a contrast CT scan at our institute, for further evaluation. CT showed no evidence of neoplasm, thrombus or fibrotic scar in the thoracic cavity. Interestingly, although the right and left brachiocephalic veins were present, the SVC was completely absent after the confluence of the brachiocephalic veins (Fig. 1, Fig. 2B, C). Instead, there were prominent collateral pathways such as azygos-hemiazygos, internal and external mammary thoracic, lateral thoracic collateral, pericardiophrenic, and caval-superficial-umbilical-portal pathways. (Fig. 2A, D, E, 3A and B). Contrary to complete absence of SVC, the inferior vena cava of this patient was intact (Fig. 2D). Both the transthoracic echocardiography and pulmonary function test showed unremarkable results. We planned a superior vena cavography, but the patient rejected any further evaluation.
Discussion
Limitation of blood flow through the SVC can cause dyspnea, fullness of breathing, cough, hemoptysis, chest pain, swelling of head and upper extremities, headache, and even cerebral edema, which are clinically defined as the SVC syndrome. For evaluation of SVC abnormalities, although non-invasive CT scan is the initially preferred imaging modality nowadays,3) conventional venography still remains an important alternative when intervention is warranted.3)4)
The common etiologies for SVC syndrome include infectious diseases (e.g. syphilitic aortic aneurysm) and malignancies (e.g. lung cancer or lymphoma). With increasing use of central venous catheter and implantable cardiac devices, thrombosis in the central vein also becomes a prevalent cause of SVC syndrome.3) Since this patient denied any medical history that may have caused SVC obstruction along with the CT images, congenital agenesis of SVC was the more likely cause than secondary obliteration. As a shallow structure linked to the right atrium might be a trace of SVC (Fig. 1), however, we cannot completely exclude the possibility of chronic SVC obstruction.
Congenital absence of SVC is a rare cause of SVC syndrome. In previous reports,5)6) patients with an absence of the right SVC were almost always related with a persistence of left SVC. Complete absence of both SVC is very rare and usually accompanied by other congenital anomalies of the heart, including cardiac conduction system, or thoracic duct system.2)7)8) Most patients with complete absence of SVC complained of various symptoms and signs related to the accompanied abnormalities and SVC syndrome, with a varying degree of severity.9)
Cough is observed in half the patients with SVC obstruction. However, the patient had none of the other above mentioned symptoms; thus, it is less likely that cough is related to SVC obstruction.1)3)
The severity of the SVC syndrome is known to be dependent on the rapidity of SVC occlusion and the development of collateral vessels. In our case, the patient had no other anomalies or medical history, except for the absence of SVC. He also showed prominent collateral vessels, which might have started to develop in the fetal period. These well-developed collateral vessels allowed sufficient venous return and made the patient asymptomatic, even in the complete absence of bilateral SVC.


 XML Download
XML Download