

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cigarette smoking is a strong risk factor in coronary artery spasm (CAS), a well-known endothelial dysfunction. CAS plays an important role in the pathogenesis of vasospastic angina (VSA) and acute coronary syndrome (ACS); it also seems to be associated with other adverse clinical outcomes.1)2)3) Several theories suggest that CAS could initiate atherosclerotic lesion development in the coronary artery.4) Due to its strong association with endothelial dysfunction, cigarette smoking is known to markedly increase the risk for all forms of cardiovascular diseases such as atherosclerosis, ACS, stroke, and CAS.5)6)7)8)9) Thus, for CAS patients an intensive medical therapy and close clinical follow-up should be recommended. For CAS patients who smoke, the importance of smoking cessation should be emphasized in order to reduce the risk. However, the impact of smoking on long-term clinical outcomes (including death and myocardial infarction [MI]) in CAS patients who have had antianginal treatment, has not been studied in depth.
Subjects and Methods
Study population
A total of 5882 patients underwent coronary angiography (CAG) from November 2004 to October 2010 at the Cardiovascular Center, Korea University Guro Hospital, Seoul, South Korea. Patients without significant CAD (with less than 70% fixed stenosis by quantitative coronary angiography) were included for the acetylcholine (Ach) provocation test. Patients were excluded if they had any one of the following conditions: prior coronary artery bypass graft (CABG), prior percutaneous coronary intervention (PCI), cerebrovascular disease (CVA), advanced heart failure (New York Heart Association class III or IV), or serum creatinine ≥2 mg/dL; these conditions can be major causes of adverse cardiovascular events, and could serve as a bias for CAS. A total of 2797 eligible patients were divided into three groups: non-CAS group (n=1188), non-smoking CAS group (n=1214), and smoking CAS group (n=395) (Fig. 1).
Study definition
Non-smoking was defined as having never smoked or having been an ex-smoker. Ex-smoking was defined as having quit smoking for more than a year before the Ach provocation test. Current smoking was defined as having smoked within one-year before the Ach provocation test. Significant CAS was defined as a luminal narrowing of more than 70% during the Ach provocation test, with or without an ischemic electrocardiogram (ECG) change or chest pain. Fixed lesion was defined as having less than 70% coronary arterial stenosis. Deaths were considered to be of a cardiac cause unless a non-cardiac cause could be confirmed. Repeated CAG (mostly due to the recurrent angina) was performed in patients suffering from acute or persistent angina, despite having received adequate antianginal medication for at least 6 months since the first CAG. In this case, a physician assumed that atherosclerotic CAD may be developing or that CAS may have started developing. Major adverse cardiovascular events (MACE) were defined as a composite of total death, MI, and de novo revascularization such as PCI and CABG.
Acetylcholine provocation test
The primary investigation for CAS consisted of clinical history taking, non-invasive stress tests such as treadmill test, ambulatory ECG and stress echocardiography, followed by an invasive angiogram performed for confirmation of a significant CAD. Nitrates, calcium channel blockers, beta blockers, angiotensin-converting enzyme inhibitors (ACEI) and other vasodilators or vasoconstrictors were withheld at least 72 hours prior to performing CAG. CAS induction was tested by an intracoronary injection of Ach immediately after diagnostic angiography, by either a trans-radial or trans-femoral approach. Ach was injected in incremental doses of 20 (A1), 50 (A2) and 100 (A3) µg/min into the left coronary artery (LCA) over a 1-minute period, with 5-minute intervals up to the maximal tolerated dose, with a continuous monitoring of ECG and blood pressure. Routine Ach provocation test of the right coronary artery was not done due to safety concerns over the higher chance of advanced AV block which requires a temporary pacemaker for maintaining an adequate Ach infusion rate and subsequent cost-effectiveness for diagnosis and management of significant CAS. Angiography was repeated after each Ach dose until a significant focal or diffuse narrowing of more than 70% was observed. An intracoronary infusion of 0.2 mg nitroglycerine was administered after completing the Ach provocation test, and angiography was performed 2 minutes later. If a significant focal or diffuse vasoconstriction (>70%) of the coronary artery was induced at any dose, the Ach infusion was stopped. End-systolic images for each segment of the LCA were chosen according to the corresponding points on the electrocardiographic traces (QRS onset or end of T wave), and analyzed using a proper quantitative coronary angiographic (QCA) system of the catheterization laboratory (FD-20, Phillips, Amsterdam, The Netherlands). The diameter of the coronary artery was measured by QCA before and after the administration of Ach at the site that showed the greatest change following the drug administration. Reference vessel diameter was measured at the proximal and distal portions of each artery. A mean reference vessel diameter was used to assess the diameter narrowing by QCA. During CAG and Ach provocation test, significant CAS was defined as a significant abnormal constriction of an epicardial coronary artery resulting in a transient myocardial ischemia. Myocardial bridge (MB) was considered when the characteristic phasic systolic compression of the coronary artery had greater than 30% decrease in diameter on the angiogram after an intracoronary nitroglycerin infusion, mostly in the anterior-posterior cranial or right anterior oblique cranial projections.
Medications
After diagnosis, CAS patients were prescribed with anti-anginal medications such as nitrate, calcium channel blockers including diltiazem and/or nicorandil, for at least 6 months, depending on a physician's discretion.
Statistical analysis
All statistical analyses were performed using SPSS 20 (SPSS Inc., Chicago, IL, USA). For continuous variables, differences among the three groups were evaluated by ANOVA or Kruskal-Wallis, and post-hoc analysis between two groups were evaluated by Hochberg or Dunnett-T3 test. Data were expressed as mean ± standard deviation. For discrete variables, differences among the three groups were expressed as counts and percentages, and analyzed with χ2 or Fisher's exact test, as appropriate. Multivariable Cox-proportional hazards regression, which includes baseline confounding factors, was used for assessing independent impact factors. We evaluated all available variables that could be of potential relevance: age, sex, cardiovascular risk factors (hypertension, diabetes, dyslipidemia, current smokers and current alcoholics, coronary fixed lesion) and MB. Various clinical outcomes were estimated with the Kaplan-Meier curved analysis, and differences among the groups were compared with the log-rank test. A two-tailed p-value of <0.05 was considered to be statistically significant.
Study endpoints
The incidence of major clinical end points such as death, cardiac death, PCI, MI, CVA, repeated CAG and MACE, were evaluated for 3 years. In this study, all patients completed a 3-year clinical follow-up through face-to-face interviews at the outpatient clinic, medical chart review, and telephone contacts. Mean follow-up period was 1095 days and clinical data from all enrolled patients were accessible for follow-up.
Results
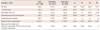
There were considerable differences in baseline characteristics such as age, sex, and alcohol history among the three groups. Compared to the non-CAS group, the smoking CAS group consisted of more males and current alcoholics. Compared to the non-smoking CAS group, the smoking CAS group consisted of more males and alcoholics (Table 1). Also, there were significant angiographic differences. In comparison to the non-CAS group, the smoking CAS group had significantly higher incidence of fixed lesion, baseline spasm, myocardial bridge, and ECG changes (including ST-segment depression, ST-segment elevation, and T-inversion). However, no difference was observed between the non-smoking CAS group and smoking CAS group (Table 1).
There was no difference among the three groups regarding individual and composite hard endpoints such as death, MI, de novo PCI, CVA, and MACE. However, soft endpoints such as recurrent angina requiring follow up CAG, occurred at a higher incidence in both the non-smoking CAS group and smoking CAS group compared to the non-CAS group (Table 2). Kaplan-Meyer curve analysis showed that in comparison to the non-CAS group, both the non-smoking CAS group and smoking CAS group showed cumulatively higher incidences of recurrent angina. However, there was no difference in recurrent angina incidence between the non-smoking CAS group and smoking CAS group (Fig. 2A).
A multivariable Cox-proportional hazards regression analysis showed that the smoking CAS group had a higher incidence of recurrent angina as compared with the non-CAS group (HR; 2.46, 95% CI; 1.46-4.14, p=0.001) and non-smoking CAS group (HR; 1.76, 95% CI; 1.08-2.87, p=0.021) for the duration of the study. However, there was no difference in recurrent angina incidence between the non-CAS group and non-smoking CAS group (Fig. 2B).
Discussion
The main findings of this study were as follows: 1) regardless of history of cigarette smoking, the CAS group did not show an increased incidence of MACE compared with the non-CAS group during the 3-year follow-up period. 2) the cigarette smoking CAS patients experienced a significantly higher incidence of recurrent angina requiring follow up CAG, as compared with both the non-CAS group and non-smoking CAS group.
In the present study, we hypothesized that cigarette smoking would adversely affect long-term clinical outcomes even with optimal medical therapy in CAS patients, as proved by the Ach provocation test. CAS patients were managed with anti-anginal medications for at least 6 months at an individual physician's discretion. Despite optimal medical therapy, we wanted to evaluate the impact of cigarette smoking on the long-term clinical course of CAS patients.
Smoking is well-known to induce significant physiological stress on the vasculature. Brunner et al.10) listed vascular damages caused by smoking, such as decreased coronary blood flow and myocardial oxygen delivery, adverse effects on lipids, blood pressure, insulin resistance, and decreased activity of endothelial nitrous oxide (NO) systems. Sugiishi and Takatsu6) reported that smoking causes dose-dependent, potentially reversible impairment of the endothelium-dependent arterial dilation in asymptomatic young adults. Smoking is closely correlated with inflammation as well.11) Inflammation is a well-known aggravating factor for endothelial dysfunction. Park et al.12) reported that a higher CRP level was associated with a higher incidence of CAS, poorer angiographic characteristics and ischemic ECG change. Takaoka et al.13) reported their findings from Japanese CAS patients with or without organic stenosis. Risk factors for CAS differed significantly from those for atherosclerosis-based coronary stenosis. However, cigarette smoking was a significant risk factor for both CAS and coronary stenosis. Also, Figueras et al.14) reported their findings from a 12-year follow-up of 273 variant angina patients. Age and old MI paired with cigarette smoking (hazard ratio [HR]; 2.39, 95% confidence interval [CI]; 1.1-5.2, p=0.027) were predictors of total mortality.
Our previous study reported15) that patients with significant CAS did not show an increased incidence of major adverse clinical outcomes compared to patients without CAS, for at least up to 5 years. The present study similarly showed that regardless of history of cigarette smoking, patients with significant CAS did not show any difference in the incidence of individual and composite hard endpoints such as death, MI, de novo PCI, CVA, and MACE (Table 2). These results may be attributed to CAS patients being prescribed with anti-anginal medications for at least 6 months, and all patients having received disease modifying medications for hypertension, dyslipidemia, diabetes, and others depending on a physician's discretion during the follow-up period. Also, since patients with serious risks (those with significant CAD, prior CABG, prior PCI, prior CVA, advanced heart failure or serum creatinine ≥ 2 mg/dL) were excluded from the study, the study groups were expected to have no significant differences in major hard endpoints. In addition, the duration of the study, which lasted for 3 years, was not extensive enough to attain statistically meaningful results in the incidence of hard-endpoints.
However, the incidence of soft-endpoints of this study, namely recurrent angina requiring follow up CAG, was significantly higher in the smoking CAS group compared with both the non-CAS group and non-smoking CAS group. Also, regardless of the smoking status, the CAS group had a significantly higher incidence of recurrent angina than the non-CAS group (Fig. 2A). However, after baseline adjustment by multivariable Cox-proportional regression analysis, the only remaining difference was the higher incidence of recurrent angina in the smoking CAS group compared with both the non-smoking CAS group (HR; 1.76, 95% CI; 1.08-2.87, p=0.021) and non-CAS group (HR; 2.46, 95% CI; 1.46-4.14, p=0.010), for up to 3 years (Fig. 2B). Most of the patients who underwent a follow-up CAG did not develop a significant CAD, and showed similar findings of significant vasoconstriction with the first index CAG findings.
The results of the present study show that there was no significant difference in major hard endpoints. However, we carefully propose that quitting of smoking paired with intensive medical therapy and clinical follow-up would help to prevent recurrent angina and hard endpoints. As shown in Table 1, all CAS patients were prescribed with anti-anginal medications. Also, the non-CAS group and the non-smoking CAS group had no difference in MACE (Table 2) and recurrent angina up to 3 years in the multivariable Cox-proportional regression analysis (HR; 1.39, 95% CI; 0.94-2.04, p=0.090, Fig. 2B).
Bakhru and Erlinger16) reported that five years after smoking cessation, the level of inflammatory markers associated with heart disease were shown to return to that of a non-smoker. Haustein et al.17) described that many pathophysiological changes caused by smoking can be reversed or improved by quitting smoking. For example, nicotine replacement therapy (NRT) trial showed that hemorheology parameters such as plasma fibrinogen, reactive capillary flow, and transcutaneous partial oxygen tension, improved significantly; other CVD risk factors such as hematocrit and white blood cell count also decreased to a greater extent in abstainers as compared with relapsers. Therefore, quitting smoking will improve clinical symptoms and reduce future cardiovascular risks in patients with VSA.
Study limitations
In this study, there were several limitations. First, smoking status was assessed at the time of the Ach provocation test. It is important whether patients in the smoking CAS group continued or discontinued smoking during the follow-up period. Other well-designed prospective studies are necessary to derive a definite conclusion. Second, medication history is very important for further detailed analyses. However in this study, the medication sub-type and duration were not demonstrated clearly due to retrospective analysis design. Third, the present study is analyzed retrospectively, and multivariable Cox-proportional regression analysis was performed to minimize the confounding factors which might have influenced the results. Also, the registry was designed with an all-comer prospective registry from 2004. We could not adjust all the limiting factors not included in the medical records or collected through telephone contact. Also, data could not be collected on anti-anginal treatment during follow-up. Medication history is very important for a detailed analysis, but prescription type, duration for which the prescriptions were given, and change in prescriptions were too broad and complex to analyze. However, all patients received anti-anginal treatment until free of angina symptoms and clinical remission, but medication type and duration were at the discretion of the individual physician.
In conclusion, regardless of cigarette smoking history, patients with significant CAS did not show an increased incidence of major adverse clinical outcomes compared with patients without CAS. However, the cigarette smoking CAS group experienced significantly more recurrent angina during the 3-year follow-up compared to the non-smoking CAS group and non-CAS group. Therefore, cessation of smoking, paired with intensive medical therapy and clinical follow-up, is highly advisable to prevent recurrent angina.



 XML Download
XML Download