

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Fractional flow reserve (FFR) is an invasive physiologic assessment of significant ischemia and is an important tool to determine whether to proceed with percutaneous coronary intervention (PCI) of intermediate coronary stenosis.1) Moreover, PCI of coronary stenosis with FFR is greater than either 0.75 or 0.80 without intervention has been safe and cost-effective.2)
On the other hand, intravascular ultrasound (IVUS) has been widely used to assess coronary stenosis, either quantitatively or qualitatively. IVUS has been reported to improve clinical outcomes compared to PCI guided by angiography alone.3) Meanwhile, IVUS-derived minimal lumen area (MLA) has been proposed as a simple anatomic alternative to FFR to determine the severity of intermediate coronary stenosis.4) Although MLA <4.0 mm2 has been widely used to predict the functional significance of stenosis in non-left main coronary artery,4)5) reported IVUS-derived MLA cutoff threshold ranges from 2.0 to 4.0 mm2 and the use of IVUS to guide PCI, has resulted in unnecessary stenting approximately half of the time because of a relatively low positive predictive value.6)
In order to elucidate whether MLA derived from IVUS can be used as an indicator in the diagnosis of functionally significant coronary artery stenosis, we conducted a systematic review and meta-analysis of studies evaluating the diagnostic accuracy of IVUS-derived MLA for the assessment of intermediate coronary lesions.
Subjects and Methods
Data sources and searches
We identified relevant studies through electronic searches of PubMed and Ovid MEDLINE and the Cochrane Central Register of Controlled Trials through January 2015. A systematic search was performed with the Medical Subject Headings terms and title/abstract words: ("Ultrasound" [Mesh] OR "Ultrasound [Title/Abstract] OR "Ultrasonography [Mesh]" OR "Ultrasonography" [Title/Abstract] OR "Ultrasonics" [Mesh] OR "Ultrasonics" [Title/Abstract]) AND ("Fractional" [Title/Abstract] AND "Flow" [Title/Abstract] AND "Reserve" [Title/Abstract]).
Study selection
Two investigators (J.-S.J. and H.-Y.J.) independently inspected the title and abstract of each citation to identify those studies reporting the diagnostic value of IVUS-derived MLA and then obtained the full text. Inclusion criteria for the primary studies were as follows: 1) studies which measured IVUS and FFR in the same set of patients at the time of coronary angiography or PCI 2) studies providing diagnostic performance test data and 3) establishment of best cut-off value for MLA based on diagnostic tests.
Quality assessment
Two reviewers (J.-S.J. and H.-Y.J.) used 11 items from the published quality assessment for studies of diagnostic accuracy (QUADAS) guidelines recommended by The Cochrane Collaboration Methods group, regarding screening and diagnostic tests as a tool to assess the included studies (Supplementary Fig. 1 in the online-only Data Supplement).7) Disarrangements were resolved by consensus.
Data synthesis and analysis
A random effects model was used to differentiate the predictive accuracy of IVUS-MLA between different studies because of variability between studies. We applied likelihood ratios (LR) for alternative statistics to sensitivity and specificity in summarizing the properties of a prognostic test.8) In the context of our analysis, the LR describes how many times likely patients who have a functionally significant CAD have that result than patients without a significant CAD. Because cut-off points of FFR for defining a functionally significant CAD were different across studies, we calculated the Spearman's correlation coefficient between sensitivity and specificity. We used diagnostic odds ratio (DOR) to describe the odds of positive test results in participants with functionally significant disease compared with the odds of positive test results in those without significant disease.
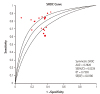
Additionally, sensitivities and specificities were summarized using a receiver operating characteristic (ROC) curve, where the diagnostic accuracy is shown by plotting 1-specificity against specificity. To summarize the curve, the area under the curve and the Q point (Q*) index were used. The point of Q (Q*, sensitivity=specificity) obtained from the summary ROC curve was used as a measure of global accuracy.9)
A chi square test was used to detect statistically significant heterogeneity. Statistical heterogeneity across studies was quantified with the Cochran's Q and I2 statistic, which is derived from Cochran's Q and the degrees of freedom [I2=100%×(Cochran Q –degrees of freedom)/Cochran Q].10) We conducted subgroup- and meta-regression analyses to detect the heterogeneity between studies. To evaluate the statistical outcome variability, we detected the pooled outcomes by sensitivity analyses.
All statistical analyses were performed using the Review Manager version 5.1 (The Nordic Cochrane Center, Copenhagen, Denmark) and Meta DiSc version 1.4 (Romany Cajal Hospital, Madrid, Spain) programs.
Results
A total of 331 publications were reviewed and 28 studies were selected for inclusion and further evaluated. Three studies were excluded because the left main coronary artery lesions were primarily evaluated. These left main studies suggest that MLA values from 4.1 to 5.9 mm2 can predict functional significance of left main disease with an FFR cut point of 0.75 or 0.80.11)12)13) Seventeen non-left main clinical studies were subsequently included into the final analysis (Fig. 1).
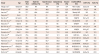
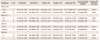
Characteristics of the included studies are summarized in Table 1. A total of 3920 patients and 4267 lesions were included in the analysis. Three studies were retrospective observational studies14)15)16) and 14 studies were prospective cohort studies with consecutive patients.4)5)6)17)18)19)20)21)22)23)24)25)26)27) Ten studies were done in patients with Asian ethnicity,4)6)14)16)17)18)22)23)25)27) whereas six studies were performed in the Western patient population.5)15)19)20)21)24) One study enrolled patients from both regional groups.26) The FFR cut-off values defining functionally significant coronary stenosis were <0.75 in three studies4)5)17) and <0.80 in 13 studies.6)14)15)16)18)20)21)22)23)24)25)26)27) One study used both FFR cut-off values for different IVUS-derived MLA.19) The weighted overall mean MLA cut-off value was 2.58 mm2 ranging from 2.00 to 4.00 mm2. To compare possible differences between studies, the prevalence of risk factors (diabetes, hypertension, hyperlipidemia, current smoking), distribution of involved coronary arteries, left ventricular ejection fraction, and proportion of patients with acute coronary syndrome were extracted (Table 2).
When all the trials were pooled, the pooled sensitivity of MLA predicting functionally significant coronary stenosis was 0.75 (confidence interval [CI]: 0.72 to 0.77; I2=78.9%) and specificity was 0.66 (CI: 0.64 to 0.68; I2=67.4%). The positive LR was 2.33 (CI: 2.06 to 2.63; I2=67.2%) and LR (-) was 0.33 (CI: 0.26 to 0.42; I2=79.4) (Fig. 2). The pooled DOR was 7.53 (CI: 5.26 to 10.76; I2=77.6; Fig. 3) and the area under the summary ROC curve for all the trials was 0.782 with the Q* of 0.720 (Fig. 4).
Sub-group and meta-regression analyses
Stratified analysis according to different FFR cut-off values revealed a trend of better diagnostic performance with trials using an FFR cut-off of 0.75 compared with trials using an FFR value of 0.80 (DOR: 21.61; CI: 10.59 to 44.11 vs. DOR: 6.59; CI: 4.62 to 9.39).
Subgroup analysis of trials performed in Asian populations revealed a DOR of 8.46 (CI: 5.92 to 12.10), whereas that of trials in Western populations was 5.37 (CI: 3.49 to 8.27). In addition, diagnostic performance of IVUS-MLA was increased in studies with QUADAS scores ≥7 (DOR: 8.76; CI 5.27 to 14.56) compared to studies with QUADAS scores <7 (DOR: 6.80; CI: 4.24 to 10.92) (Table 3).
Possible sources of heterogeneity across the studies were explored using meta-regression analysis with five covariates as predictor variables: FFR cut-off values, MLA cut-off values, QUADAS score, study design, and ethnicity of the involved patients. An FFR cut-off of 0.75 was associated with four times higher diagnostic accuracy compared to the value of 0.80 (relative DOR: 3.92; 95% CI: 1.25 to 12.34; p=0.023).
Discussion
In the present meta-analysis of 17 observational studies, consisting of 3920 patients, we found that IVUS-derived MLA has a limited but acceptable pooled diagnostic performance in predicting functionally significant non-left main coronary artery disease with a pooled DOR of 7.53 and the area under the summary ROC curve of 0.782. Furthermore, we found that the diagnostic performance of IVUS-derived MLA was higher in Asian population studies when compared to studies performed in Western populations. We also found that an FFR cut-off of 0.75 is associated with better diagnostic accuracy compared to an FFR cut-off of 0.80.
Despite promising data about the use of anatomical variables to correlate the functional significance of coronary stenosis, most physicians do not believe that anatomical predictors can substitute for FFR. Even though IVUS has excellent spatial resolution and provides information to guide intervention, lumen assessment alone does not reflect microcirculatory function, collateral circulation, and viability of the corresponding myocardium.28) Nevertheless, many physicians use IVUS to guide interventional treatment in lieu of FFR for several reasons. The FFR test requires additional equipment and expert personnel to measure and interpret the results. Contrary to FFR, IVUS is relatively simple to perform and its use is associated with low complication rates. In addition, the operators do not need to use intracoronary adenosine to induce maximal hyperemia, which puts the patient at risk. Although the diagnostic accuracy of IVUS is not enough to substitute for FFR, both IVUS and FFR may be used as complementary tools in the catheterization laboratory to provide both functional and anatomical data to guide optimal decision-making in patients with intermediate coronary stenosis.
Previous meta-analysis comparing IVUS-MLA versus FFR for the assessment of intermediate lesions revealed limited accuracy of IVUS imaging in non-left main lesions to predict functionally significant stenosis as compared with FFR, while better accuracy was shown in left main lesions.29) The results of our study support data generated by a previous study. However, we included and analyzed data from several other recently published studies.15)16)22)23)24)25)26)27) We did not include studies performed exclusively on left main disease subsets because we thought that left main stenosis has a different clinical meaning with different IVUS-MLA cut-offs compared with other vessels. Therefore, left main disease needs to be assessed separately. In addition, we performed several subgroup analyses according to FFR cut-off values, MLA, ethnicity, and QUADAS scores of the included studies to better understand and confirm benefits in certain subgroups compared with others.
Contrary to the earlier reports using an FFR cut-off value of 0.75 to define functional significance of coronary narrowing.4)5)17) Recent studies adopted a less restrictive and more clinically relevant cutoff value of 0.80 to minimize the number of untreated lesions that may cause significant ischemia.6)18)30) Even though subgroup- and meta-regression analysis of our study suggests greater diagnostic performance of IVUS-derived MLA in studies using an FFR cut-off point of 0.75 compared to studies using 0.80, it is not appropriate to adopt 0.75 as the standard cut-off point for functionally significant coronary disease. This is due to routine measurements of FFR and stenting limited to stenoses with an FFR ≤0.8, which significantly lowered the rate of the composite endpoint of death, myocardial infarction, and repeat revascularization at one year compared with stenting of all of the lesions deemed appropriate based on the angiography.30)
In our analysis, mean MLA cut-off in Asian populations was 2.68 mm2 and that of Westerners was 3.03 mm2. The difference in mean MLA cut-off value by ethnicity is one of the interesting and novel findings in our study. Han et al.26) found different demographic and lesion characteristics, as well as, different cut-off values between Asians and Westerners. We postulated that lower body mass index and smaller myocardial masses in Asian people may result in lower MLA cut-off values and different physiologic significance of coronary stenosis when compared with Western populations.
There are several limitations to be addressed in our study. First, the majority of studies included in our analysis were observational studies from different cohorts with no randomized controlled trials. This caused our results to have insufficient power. Second, the proportion of the involved coronary arteries and extent of coronary diseases were different across the included studies. It was not possible to suggest the diagnostic performance of IVUS-MLA according to the lesion location. Further, we could not perform separate subgroup analyses of all coronary arteries and their location (proximal-, mid-, distal-) because very few studies presented such data. Moreover, we could not differentiate patients presenting with stable angina and acute coronary syndrome, despite differences in clinical significance of IVUS-derived MLA and FFR. Additionally, the IVUS criteria to discriminate the functional significance of lesions in different locations were applied differently across studies. Last, we did not take into account the plaque composition that can affect clinical outcomes.
In conclusion, IVUS-derived MLA has limited diagnostic accuracy in predicting functionally significant coronary artery disease and cannot be used alone to make the decision whether or not to proceed with the PCI of intermediate non-left main coronary artery stenosis.




 XML Download
XML Download