

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Central venous catheterization with a large-bore catheter is widely used to gain vascular access while performing hemodialysis or continuous renal replacement therapy. Arterial misplacement of the hemodialysis catheter can occur despite ultrasound guidance1) and can lead to serious complications including hematoma, hemothorax, pseudoaneurysm, arteriovenous fistula, or stroke due to an intra-arterial thrombus.2) Open repair is a safe choice for management, but the site of arterial injury is potentially difficult to expose surgically. Additionally, underlying comorbidities can make surgical operations difficult for critically ill patients.3) Here we report a case of an inadvertently catheterized subclavian artery with an 11.5-French large-caliber hemodialysis catheter and successful percutaneous repair using suture-mediated closure devices and a temporary balloon tamponade.
Case
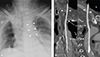
A 57-year-old man with decompensated liver cirrhosis underwent liver transplantation. Massive bleeding occurred during and after the operation, and the total estimated blood loss was approximately 25 L. Despite resuscitation with intravenous fluids and transfusions, he became anuric, and the transplant surgeons decided to start continuous renal replacement therapy. A temporary 11.5-French, dual-lumen, Mahurkar™ catheter (Covidien, Mansfield, MA, USA) was placed at the left internal jugular vein, but the tip of the catheter appeared to lie within the descending thoracic aorta in the chest X-ray (Fig. 1A). Computed tomography angiography revealed that the catheter had penetrated the vessel wall of the left internal jugular vein and entered the left subclavian artery, extending into the descending thoracic aorta (Fig. 1B and Video in the online-only Data Supplement). Considering the burden of general anesthesia and the need for thoracotomy or partial removal of the first rib during surgery, the patient was referred to us for endovascular repair of the subclavian artery. After acquisition of informed consent from the patient and family members, the patient was moved to a hybrid room that allowed intervention and open surgery to be performed.
The left upper chest, neck, and right groin area were prepared in a sterile fashion, and an 8.5-French sheath was placed in the right common femoral artery. Angiography revealed malposition of the catheter in the left subclavian artery with an insertion site close to the origin of the left vertebral artery (Fig. 2A). A 0.035-inch Glidewire®, hydrophilic coated guidewire (Terumo, Tokyo, Japan) was placed through the misplaced catheter. Immediately after catheter withdrawal, balloon tamponade was performed by placing a 13-mm-diameter occlusion balloon catheter just distal to the entry site of the misplaced catheter (Fig. 2B). Despite hemostasis lasting longer than 1 hour, continuous extravasation was observed from the entry site of the misplaced catheter (Fig. 2C). We therefore decided to perform percutaneous closing of the subclavian artery using two 6-French Perclose Proglide® (Abbott Vascular, Redwood, CA, USA) devices, the largest of such devices available in Korea. Balloon tamponade was performed at the proximal part of the subclavian artery using a 10-mm-diameter, 20-mm-long, Armada™ 35 percutaneous transluminal angioplasty catheter (Abbott Vascular, Redwood, CA, USA). The angioplasty catheter was 1 mm less in caliber than the subclavian artery in order to minimize bleeding during removal of the malpositioned catheter and reintroduction of the Perclose Proglide® through the guidewire. A Perclose Proglide® device was advanced over the guidewire, medially rotated by approximately 30°, and then deployed (Fig. 3A). The strands were left outside of the body and tagged with a small clamp. Guidewire access was maintained, and a second Perclose Proglide® device was inserted, laterally rotated 30°, and deployed. While maintaining guidewire access, the knots of the two sutures were cinched over the guidewire. Due to the persistence of mild extravasation, a third Perclose Proglide® device was deployed before removal of the guidewire. The balloon catheter was exchanged for a 20-mm-diameter occlusion balloon catheter, which remained inflated for longer than 20 minutes just distal to the site of extravasation (Fig. 3B). Final angiography showed no extravasation of contrast, confirming successful closure of the subclavian artery (Fig. 3C). The patient was discharged 45 days after the procedure without any complications.
Discussion
Accidental arterial puncture occurs in approximately 2.7% of subclavian approaches.4) There is an increased risk of serious complications such as active hemorrhage and pseudoaneurysm formation if catheter removal is attempted at a non-compressible site. Inadvertent subclavian artery catheter insertion can be treated by surgical or endovascular techniques or with a combination of these approaches. Both critically ill patients and those with coagulopathies have limited endovascular options and are poor candidates for surgical treatment. Stent grafts are known to have 94-100% success rates for treatment of inadvertent subclavian artery catheter placement.5) In Korea, stent grafts are covered by health insurance and are cheaper than percutaneous closure devices. Although stent graft placement at the subclavian artery presents the risk of vertebral artery occlusion, it is possible to deploy a stent graft without vertebral artery occlusion by following the digital subtraction angiography "road map". If the right vertebral artery was dominant and patent, posterior circulatory territory could not be compromised despite occlusion of the left vertebral artery. However, in our patient, the line pierced the subclavian artery close below the left clavicle, and stent fracture or compression could occur between the first rib and clavicle. Using angiography, an observation study reported significant stenosis (20%) and occlusion (12%) during a 10-year period.6) In addition, long-term antiplatelet therapy could increase the bleeding risk in patients with recent massive bleeding and liver transplantation. Balloon tamponade offers technically feasible and effective hemostasis, but prolonged balloon dilatation can lead to limb ischemia, thromboembolism, and delayed pseudoaneurysm formation.7) Furthermore, this instrument is difficult to seal within large puncture sites such as in our patient.8)
After invasive procedures, the use of percutaneous closure devices via the femoral artery is recommended to achieve faster hemostasis and allow earlier patient mobilization9) The off-label application of these devices in inadvertently catheterized subclavian arteries has been described previously, where serious complications arose including device failure, infection, incomplete hemostasis, pseudoaneurysm, and embolic stroke.10) We has also experienced a case of embolic stroke possibly from thrombi around the misplaced catheter. We believe that it is helpful to explore the thrombi using pre-procedural ultrasound and to use heparin with monitoring of the activated clotting time. One previous case of a misplaced subclavian catheter with a diameter larger than 11 French was successfully repaired using a 10-French Prostar XL® (Abbott Vascular, Redwood, CA, USA) device and a temporary balloon tamponade.11) The Prostar XL device® deploys 4 needles and is commonly used for closing arterial access sites for catheter sizes up to 18-French using the preclosure technique. The 6-French Perclose Proglide®, which is the largest size available in Korea, deploys 2 needles and is certified for use in 5- to 21-French access sites. For access sites larger than 8-French, at least two devices and the preclosure technique are required.12) However, it is impossible to close an inadvertently catheterized subclavian artery using the preclosure technique. Therefore, we used a balloon tamponade at the proximal part of the subclavian artery in order to minimize the risk of bleeding, and hemostasis was achieved by the sequential implementation of three 6-French Perclose Proglide® devices, instead of a 10-French Prostar XL® device.
In conclusion, we report a case of inadvertent subclavian artery catheterization with an 11.5-French, large-caliber hemodialysis catheter that was successfully repaired percutaneously using suture-mediated closure devices and a temporary balloon tamponade. The procedure was performed without embolic neurological complications. Sequential implementation of suture-mediated closure devices with a temporary balloon tamponade backup can be considered as a reasonable alternative for poor surgical candidates with inadvertent arterial catheterization at non-compressible sites.


 XML Download
XML Download