

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Hypertension (HT) is a major global public health burden,1) and it is an important risk factor for cardiovascular disease (CVD) and cerebrovascular accident.2) Prehypertensive subjects are at risk of progression to HT, and prehypertension is associated with excessive morbidity and mortality due to CVD.3) Echocardiography is an important non-invasive diagnostic tool for investigation of left ventricular function. Left ventricular diastolic dysfunction due to various myocardial diseases occurs frequently in hypertension, and it is a common cause of heart failure in patients with hypertension.4) However, few studies have shown an association between diastolic dysfunction grade and blood pressure classification, especially mild hypertension or prehypertension (preHT). We sought to investigate the association between diastolic dysfunction and preHT in apparently healthy middle-aged adults.
Subjects and Methods
Study population and protocol
The present study included 4261 Koreans (male:female ratio 7:3), 45 to 64 years of age with no previous history of HT, diabetes mellitus, malignancy, proven coronary artery disease, or valvular heart disease, who underwent routine health examinations including echocardiography at the Health Promotion Center of Samsung Medical Center from January 2009 to June 2010. This study was approved by the Samsung Medical Center Institutional Review Board, and the requirement for obtaining informed consent was waived for this retrospective study.
Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured after the subject had rested for ten minutes in the sitting position. Blood samples were collected from the antecubital vein after overnight nil per os (NPO). Total cholesterol (TC), triglyceride (TG), high density lipoprotein-cholesterol (HDL-C), low density lipoprotein-cholesterol (LDL-C), fasting blood sugar (FBS), and serum creatinine (Cr) levels were measured. The estimated glomerular filtration rate (Egfr) was calculated using the Chronic Kidney Disease Epidemiology Collaboration(CKD EPI) equation. Information on the presence of HT, type 2 diabetes mellitus, and history of smoking and alcohol consumption was obtained from personal questionnaires.
Echocardiographic evaluation
Subjects underwent comprehensive transthoracic echocardiography (2-dimensional, M-mode, and tissue Doppler echocardiography) using commercially available equipment (Vivid 7, GE Medical Systems, Milwaukee, WI, USA). Well-trained echocardiographers interpreted all echocardiograms and obtained the following measurements: left ventricle internal dimension measured at end diastole (LVIDd), left ventricle internal dimension measured at end systole (LVIDs), interventricular septal wall thickness at end diastole (IVSd), left ventricle posterior wall thickness at end diastole (LVPWd), and left ventricular mass index (LVMI), left ventricular mass divided by body surface area (BSA), height (cm)0.725×weight (kg)0.425×0.007184 measured with M-mode; early diastolic mitral inflow velocity/late diastolic mitral inflow velocity (E/A), early diastolic mitral inflow velocity/peak early diastolic mitral septal annular velocity (E/e') measured by flow and tissue Doppler analysis; left ventricular ejection fraction (LVEF) measured on 2-dimensional (2-D) echocardiography using biplane Simpson's method; and left atrial volume index (LAVI) measured on 2-D echocardiography calculated by the area-length method and indexed to BSA. Left ventricular diastolic dysfunction was categorized as normal, grade 1, grade 2, grade 3, or grade 4 according to the guidelines of the American Society of Echocardiography. All echocardiographic data were measured and obtained in accordance with the American Society of Echocardiography guidelines and the European Association of Echocardiography guidelines.5)6) Unless otherwise specified in this paper, diastolic dysfunction referenced herein refers to left ventricular diastolic dysfunction.
Blood pressure classification
PreHT was defined as SBP of 120-139 mmHg and/or DBP 80-89 mmHg according to the Seventh Report of the Joint National Committee (JNC7)7) criteria and without the use of any antihypertensive drug and/or non-pharmacological interventions. HT was defined as SBP≥140 mmHg and/or DBP≥90 mmHg and/or with active antihypertensive drug therapy. If subjects had SBP≥140 mmHg and/or DBP≥90 mmHg, the blood pressure was retaken, and the mean blood pressure value was used. Normotension was defined as SBP<120 mmHg and DBP<80 mmHg without the use of antihypertensive medication. The prevalence of preHT in our study was 42.1%. This value was slightly lower than that in previous reports among Koreans, in which Jang et al. showed that the prevalence of preHT was over 50% in general Korean middle-aged adults.8)
Obesity
Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters. Obesity was defined as BMI≥25.9)
Health behavioral factors
Subjects were identified as current smokers if they had smoked within one year of the survey date and as former smokers if they had not smoked for at least one year before the survey date. Alcohol drinking was defined as current drinking within one year of the survey date as reported in the health interview questionnaire.
Statistical analyses
The general characteristics analyses among HT, preHT and normotension groups were performed using one-way analysis of variance (ANOVA) and Bonferroni method in multiple comparisons testing for the continuous variables and χ2 tests for the categorical variables. Multinomial logistic regression analysis was conducted to show the associations among HT, preHT and normotension and diastolic dysfunction adjusted for variables including age, gender, smoking, BMI, TG, HDL-C, and FBS.
This study was approved by the Samsung Medical Center Institutional Review Board, and the requirement for obtaining informed consent was waived for this retrospective study (IRB File Number 2009-09-088).
Results
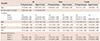
Clinical characteristics of the subjects are summarized in Table 1. Approximately 40% of our subjects were prehypertensive. The proportion of diastolic dysfunction grade 1 or 2 was significantly higher in preHT (31.0% overall) and HT (38.0% overall) groups compared to the normotensive group (19.1% overall) (p<0.01). Male gender was more prevalent in the preHT group compared to normotensive or HT groups (p<0.001). The proportion of current smokers, current alcohol drinkers, and obese subjects was significantly different among the 3 groups (p<0.001). The mean values of SBP, DBP, TC, TG, LDL-C, FBS, LVIDd, IVSd, LVPwd, E/e', LVEF, LAVI, and LVMI were higher in patients with HT than in subjects with normotension or preHT (p<0.001). The mean values of HDL-C and Cr were lower in the HT group than in the normotensive or preHT group (p=0.008, p<0.001, respectively).
Data showed that the statistically significant adjusted odds ratio (OR) for diastolic dysfunction with preHT was as follows: male gender, 1.59 (95% confidence interval [CI] 1.30-1.95); current smoking, 0.80 (95% CI 0.66-0.98); BMI, 1.14 (95% CI 1.11-1.18); and the OR was 1.66 (95% CI 1.40-1.96) for grade 1 diastolic dysfunction and 1.37 (95% CI 0.95-1.97) for grade 2 diastolic dysfunction, respectively. Particularly, in males, the adjusted OR for diastolic dysfunction with preHT was 1.74 (95% CI 1.44-2.10) for grade 1 diastolic dysfunction and 1.31 (95% CI 0.84-2.04) for grade 2 diastolic dysfunction. In females, the adjusted OR for diastolic dysfunction with preHT was 1.32 (95% CI 0.91-1.90) for grade 1 diastolic dysfunction and 1.47 (95% CI 0.76-2.76) for grade 2 diastolic dysfunction, respectively (Table 2).
Discussion
Our overall findings showed that diastolic dysfunction appears to be significantly associated with preHT in apparently healthy middle-aged Korean population. Results of the present study correspond well with those in a previous study, which showed that preHT was associated with LV diastolic function.10) The results of the present study are also consistent with another report on diastolic dysfunction and blood pressure classification in healthy Turkish adults, which showed that diastolic function was slightly impaired in prehypertensive subjects.11) In other reports, blood pressure control is known to improve diastolic dysfunction in hypertensive subjects.12)13)14) The association between diastolic dysfunction and HT has been reported previously.15)16)17) Our data showed a relatively higher grade of diastolic dysfunction in healthy middle-aged prehypertensive subjects. As diastolic dysfunction is an important pathophysiological intermediate between HT and heart failure, preventive strategies are necessary to reduce morbidity in prehypertensive subjects who show a risk for diastolic dysfunction. Examination of heart function using echocardiography has been recommended for assessing target organ damage in hypertensive patients, but our research suggests that echocardiographic examination should be extended to include prehypertensive subjects, and a more aggressive lifestyle change and/or treatment for middle-aged prehypertensive subjects may be recommended according to their heart function.
To date, few prior studies regarding the association between diastolic dysfunction and preHT according to gender have been presented. We showed an association between diastolic dysfunction and preHT, which was especially prominent in males. This is consistent with previous reports18) showing an overall higher incidence of diastolic dysfunction in healthy adult men compared to women. According to previous study19) on diastolic dysfunction in patients with HT which showed that some of the echocardiographic parameters for diastolic function demonstrated a trend towards more impaired diastolic function in male hypertensives, this finding can be explained by the relatively larger size of the mitral annulus of the heart resulting in decreased ventricular filling velocities and deceleration time. Another explanation for this finding, at least in middle-aged people, is the protective effect of female hormones, as indices of left ventricular filling showed a significant decline with age in premenopausal and postmenopausal women in a previous study.20) However, as the design of this study was retrospective and our subjects were people who voluntarily visited our health promotion center for health examinations, a well-designed, age- and gender-matched prospective echocardiographic study may be needed for classification.
The prevalence of LV diastolic dysfunction in the normotensive group in our study was approximately 20%, and an additional analysis showed a higher prevalence of LV diastolic dysfunction in the older age group (Supplementary Tables 1 and 2 in the online-only Data Supplement). As already known, LV diastolic dysfunction can develop as the age increases in the absence of heart disease including HT.21)22) In addition, higher arterial stiffness has also been reported to be associated with worse LV diastolic function.23)24) Meanwhile, there was a significant difference in BMI among the groups, and this may have been one of the mechanisms that may be associated with diastolic dysfunction in prehypertensive subjects. Fenk et al.25) showed that in severe obesity, weight reduction was associated with improved LV diastolic function, and the Northern Manhattan Study, a population-based prospective cohort study in the US, showed that increased BMI was associated with worse LV diastolic function.26)
Although prehypertensive subjects are at risk of progression to HT,27) pharmacological therapy in preHT subjects without comorbidities remains debatable with respect to whether drug treatment should be initiated. However, as our data suggest, these prehypertensive subjects are at higher risk of developing early and significant left ventricular diastolic dysfunction, and they may need to modify their health behavior such as reducing sodium intake, losing weight, and participating in regular physical activity.
Limitations of the present study
This study has several limitations. Firstly, this was a retrospective study performed on subjects who voluntarily visited our center for health examinations. Thus, we could not observe any causal relationships between diastolic dysfunction and preHT. Secondly, because echocardiography was performed in middle-aged subjects who wanted a detailed evaluation of CVD, our study may reflect some level of selection bias. However, selection bias in this study could be low because we excluded patients with previous history of HT, diabetes mellitus, or malignancy based on medical history and those with proven coronary artery disease or valvular heart disease. Finally, the proportion of males was higher than that of females in our study. To compensate for this limitation, logistic regression was performed after adjusting for gender. Although the study was conducted at a single center with asymptomatic subjects who did not have CVD, we believe that this study in a substantially large group of subjects accurately represents Korean middle-aged adults who underwent echocardiography.

 XML Download
XML Download