

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The no reflow phenomenon is a serious complication following percutaneous coronary intervention (PCI). It is defined as a state of myocardial hypoperfusion in the presence of a patent epicardial coronary artery.1)2) No reflow negatively affects the clinical outcome in patients with acute myocardial infarction (AMI),3)4)5)6) and it is associated mainly with increased mortality or left ventricular remodeling, despite its relatively low incidence.7)
The pathomechanism of no reflow includes ischemia-reperfusion injury, myocardial edema, endothelial swelling, capillary obstruction, vasospasm, inflammatory response, and distal coronary embolization.1) Although interventional cardiologists try to overcome no reflow using various methods and drugs,2) persistent no reflow often remains despite adequate revascularization of coronary stenosis. However, few studies have described the incidence and prognosis of transient or persistent no reflows in patients with AMI.8)9)10)11) Furthermore, no studies have examined the long-term clinical outcomes according to the persistence of no reflow.
Therefore, this study investigated the incidence of transient or persistent no reflow during PCI, its clinical and angiographic characteristics, and the long-term clinical outcomes in patients with AMI based on a Korean multicenter registry.
Subjects and Methods
Study population
The Convergent Registry of Catholic and Chonnam University for AMI (COREA-AMI) is a Korean prospective, multicenter, observational registry that was designed to reflect real-world practice in Korean AMI patients at nine centers with facilities for primary PCI, representing two universities, between January 2004 and December 2009. Of the 4748 patients in the COREA-AMI registry, 4329 who underwent PCI with coronary stents were analyzed. We excluded 419 patients, including 184, 17, and 97 patients without any no reflow who achieved post-procedural thrombolysis in myocardial infarction (TIMI) flow grades 0, 1, or 2, respectively, 28 patients who did not have coronary stents implanted, and 93 patients with insufficient data. The remaining subjects were divided into three groups according to the presence of no reflow and post-procedural TIMI flow grade: the normal reflow group was defined as patients without any no reflow who achieved final TIMI flow grade 3 (n=4071); the transient no reflow group was defined as patients having no reflow during PCI who achieved final TIMI flow grade 3 after adequate management of the no reflow (n=213, 4.9% of all patients); and the persistent no reflow group was defined as patients having no reflow whose final TIMI flow grade was ≤2 despite of management for no reflow (n=45, 1.0% of all patients). The no reflow phenomenon was defined as the disruption of coronary flow distal to a treatment segment following initial procedure despite patency of the epicardial coronary arteries after PCI. An operator at each center confirmed no reflow during PCI. Patients with vasospasm, distal embolism or coronary dissection were excluded. The ethics committee of each participating hospital approved the study protocol, and all patients provided written informed consent.
Study definitions and outcomes
The patients' demographics, vital signs on admission, and medical history were compared among groups. A history of renal insufficiency included a history of chronic kidney disease and patients receiving chronic dialysis. The diagnosis of ST-segment elevation myocardial infarction (STEMI) was based on ST-segment elevation>2 mm in at least two precordial leads, ST-segment elevation>1 mm in at least two limb leads, or new left bundle branch block on a 12-lead electrocardiogram in the infarct-related artery distribution, as determined by coronary angiography with increased cardiac-specific biomarkers. All laboratory findings were performed upon admission, except for lipid profiles, which were obtained after at least 9 hours of fasting within 24 hours of hospitalization. The estimated glomerular filtration rate was calculated using the Modification of Diet in Renal Disease study equation.12) Baseline left ventricular ejection fraction was determined using two-dimensional echocardiography performed before or after PCI.
Multi-vessel coronary artery disease was defined as significant stenosis (disease stenosis≥70%) of more than one epicardial coronary artery, including the culprit artery. The coronary blood flow before and after PCI was classified using the TIMI score, and coronary lesion complexity was based on the American College of Cardiology (ACC)/American Heart Association (AHA) definitions.13)14) Patients who underwent PCI were given 300 mg aspirin and 600 mg clopidogrel as a loading dose before PCI. Doses of 50-70 U/kg of unfractionated heparin were used before or during PCI to maintain the activated clotting time at 250-300 seconds. Low-molecular-weight heparin, drug-eluting stent implantation, and the overlapping stent technique were used at the discretion of the clinician. Thrombus aspiration or use of a glycoprotein IIb/IIIa inhibitor in patients with large thrombotic burdens and insertion of an intra-aortic balloon pump in patients with cardiogenic shock were also performed at the discretion of the interventional cardiologists. After PCI, 100-300 mg aspirin and 75 mg clopidogrel were prescribed daily.
The follow-up duration was 3-years after AMI. While the primary endpoint was all-cause mortality, we also evaluated the incidence of cardiac mortality, re-hospitalization due to congestive heart failure (CHF), non-fatal myocardial infarction (MI), target vessel revascularization, and stent thrombosis. Cardiac mortality was registered when a definite cardiac cause was identified; other causes of mortality were considered non-cardiac mortality. Non-fatal recurrent MI was defined as the development of recurrent angina symptoms with new 12-lead electrocardiographic changes or increased cardiac specific biomarkers. Target vessel revascularization was defined as repeated PCI for any segment of the entire coronary artery, including the segments treated using coronary stents, and stent thrombosis was defined as definite and probable stent thrombosis, according to the Academic Research Consortium definition.15)
Statistical analysis
Continuous variables are presented as the means±standard deviations and were compared using the Student's t-test or Mann-Whitney U-test. Comparisons among the three groups were performed using one-way analysis of variance. Categorical variables were analyzed using Pearson's chi-square test or Fisher's exact test to determine the significance of differences. The 3-year mortality was estimated by the Kaplan-Meier method, and curves were compared with the log-rank test. Cox-regression analysis was done to compare study outcomes between normal reflow and transient or persistent no reflow after adjusting confounding variables which were known to be associated with the study outcomes. Logistic regression analysis was performed to evaluate independent predictors of transient or persistent no reflow. Among variables predicting no reflow, clinically relevant variables with marginal significance (defined as p<0.2) in the univariate analysis were entered into multivariate models to determine predictors of transient and persistent no reflow.
All analyses were two-tailed, and all variables were considered significant when p<0.05. Statistical analyses were performed using SPSS for Windows, version 18.0 (SPSS Inc., Chicago, IL, USA).
Results
Baseline clinical characteristics
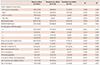
The persistent no reflow group had more STEMI patients and a lower admission blood pressure than did the other groups. The medical histories and proportions of male patients and those with a higher Killip class (≥3) were comparable among groups. The levels of creatine kinase-myocardial band isoenzyme, high density lipoprotein-cholesterol, and N-terminal pro-brain type natriuretic peptide and the prescription rates of triple antiplatelet agents and statins were higher in the no reflow group, but there was no difference between the transient and persistent no reflow groups. The persistent no reflow group had lower levels of total cholesterol, serum glucose, low-density lipoprotein-cholesterol, left ventricular ejection fraction, and were more likely to include patients who were prescribed a beta blocker and angiotensin-converting enzyme inhibitor or angiotensin-II receptor blocker (Table 1).
Coronary angiographic and procedural characteristics
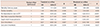
Table 2 summarizes the coronary angiographic and procedural findings. The prevalence of multi-vessel disease, B2 or C coronary lesion, and mean stent diameter were higher in the no reflow group than in the normal reflow group. The no reflow group also experienced more thrombus aspiration and insertion of an intra-aortic balloon pump and received more glycoprotein IIb/IIIa inhibitor during the procedure, while these treatments were similar for the transient and persistent no reflow groups. The persistent no reflow group had more pre-procedural TIMI flow grade 0, but less pre-procedural TIMI flow grade 3. The persistent no reflow group received more inotropics during the procedure. However, similar results were observed among groups for the distribution of the infarct-related artery, total stent length, and rate of patients receiving overlapping stents.
In-hospital outcomes and study endpoints
During the in-hospital stay, the persistent no reflow group experienced more peri-procedural cardiogenic shock and multiorgan failure and had higher in-hospital mortality than did the other groups. The persistent group had poorer outcomes in terms of in-hospital mortality, fatal ventricular arrhythmia, and cardiogenic shock than did the transient no reflow group (Fig. 1).
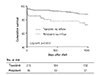
The primary endpoint occurred in 811 patients (18.7%) during the follow-up period. The persistent no reflow group had the highest all-cause (738 [18.1%] vs. 52 [24.4%] vs. 21 patients [46.7%]) and cardiac (321 [7.9%] vs. 28 [13.1%] vs. 18 patients [40.0%]) mortality rates. Between the transient and persistent no reflow groups, the persistent group had higher all-cause mortality (Fig. 2). However, the incidences of secondary endpoints did not differ among the groups (Fig. 3). Table 3 shows the adjusted risks for the study endpoints. Persistent no reflow increased the risks of all-cause mortality (hazard ratio [HR] 1.98, 95% confidence interval [CI] 1.08-3.65, p=0.028), cardiac mortality (HR 3.28, 95% CI 1.54-6.95, p=0.002), and re-hospitalization due to CHF (HR 12.05, 95% CI 4.26-34.14, p<0.001). Transient no reflow was not associated with cardiac mortality (HR 1.45, 95% CI 0.84-2.49, p=0.186), but was associated with all-cause mortality (HR 1.58, 95% CI 1.11-2.24, p=0.010), compared to the normal reflow group. Neither the transient nor the persistent no reflow group had an increased risk of non-fatal MI, target vessel revascularization, or stent thrombosis. However, the risk of early stent thrombosis (within 30 days after PCI) was higher in the persistent no reflow group.
Independent predictors of no reflow phenomenon
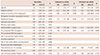
To determine independent predictors of no reflow, logistic regression analysis was performed (Table 4). Among variables predicting no reflow phenomenon, variables with p≤0.2 in the univariate model (except for use of glycoprotein IIb/IIIa inhibitor and thrombus aspiration which might be associated with management for no reflow) were tested to identify predictors of both transient and persistent no reflow in the multivariate analysis. The result determined that old age, multi-vessel disease, B2 or C lesion, and stent diameter were all related to the development of transient no reflow. However, only old age and preprocedural TIMI 0 were predictors of persistent no reflow.
Discussion
This study investigated the long-term clinical outcomes of transient or persistent no reflow in patients with AMI who underwent PCI. The principal findings of our study were that poor in-hospital and long-term outcomes were associated with persistent no reflow during PCI compared to patients with normal reflow or transient no reflow despite its low incidence. However, the transient no reflow group had lower reduced all-cause mortality only, not cardiac mortality, compared to the normal reflow group.
In this study, the incidence of the no reflow phenomenon in AMI was similar to that in a large population study.7) However, the majority of the no reflow cases was transient no reflow. The published incidence of persistent no reflow is 0.7-2.0%,8)9)16) which is comparable to our series. Several studies have investigated the impact of transient or persistent no reflow in AMI populations.8)10) Mehta et al.8) reported a low incidence of transient no reflow (1.3%) in patients with STEMI who underwent primary PCI. Patients with transient no reflow had higher in-hospital (2 vs. 13%, p=0.04) mortality compared to those with normal reflow. Data from the Melbourne Interventional Group (MIG) compared the clinical outcomes among normal reflow and transient and persistent no reflow patients undergoing PCI. Interestingly, transient or persistent no reflow increased the target vessel failure as well as mortality at the 30-day follow-up.10) Other small single-center studies reported higher short-term mortality in the persistent no reflow groups.9)11) However, few studies have compared transient and persistent no reflow in patients with AMI over the long-term.
In our study, the in-hospital and long-term mortalities were higher in the persistent no reflow group. Based on the result of 30-day mortality among groups (2.5 vs. 5.2 vs. 22.2%, p<0.001, data not shown), higher long-term mortality in the persistent no reflow group might be due to higher early mortality. Unlike other studies, transient no reflow was only associated with increased all-cause mortality in our study, not cardiac mortality. A previous study reported higher short-term all-cause or cardiac mortality in the transient no reflow group than in a normal reflow group.10) This landmark analysis showed that the transient group was associated with more in-hospital adverse cardiac events such as contrast-induced acute kidney injury, peri-procedural MI, and in-hospital mortality. In the present study, in-hospital outcomes were the same for patients with normal reflow and transient no reflow except for higher in-hospital mortality in the transient group. These differences of in-hospital outcomes might be associated with similar cardiac mortality between the normal and transient no reflow groups in our study. Furthermore, the comparison of long-term mortality between the two groups was not evaluated in prior studies. The difference in the repeat target vessel PCI outcome between our study and the prior report might result from a lower implantation rate of coronary stents, longer mean length of the implanted stents, or higher incidence of bifurcation lesions in the persistent no reflow group of the MIG study.10) The above-mentioned factors are all associated with repeat target vessel revascularization.17)18)19) Notably, our study showed that persistent no reflow increased the risk of early stent thrombosis compared with normal or transient no reflow. Brodie et al.20) evaluated predictors of early stent thrombosis and found that STEMI, small stent size, Killip class III or IV, and reperfusion time≤2 hours were all associated with the development of early stent thrombosis. In our study, the persistent no reflow group also had a higher prevalence of STEMI and higher Killip class, and these factors might increase the risk of early stent thrombosis. Although other factors related to early stent thrombosis were similar to prior reports, the reason for the correlation of shorter reperfusion time to early stent thrombosis is uncertain. Further research is needed to confirm the relation between persistent no reflow and early stent thrombosis.
Studies have established clinical and angiographic factors that predict the no reflow phenomenon in patients with acute coronary syndrome. The clinical predictors include initial shock, age, STEMI diagnosis, longer symptoms-to-admission time, and higher level of N-terminal pro brain-type natriuretic peptide.7)21)22) The angiographic factors include a complex coronary lesion based on the ACC/AHA definition, lesion length, use of a glycoprotein IIb/IIIa inhibitor during PCI, pre-procedural TIMI flow grade 0, bifurcation lesion, coronary anatomical scoring system, amount of attenuated plaque, larger necrotic core, and more thin-cap fibroatheroma on intravascular ultrasound.7)10)23)24)25) In our patients, similar factors were associated with the development of no reflow. However, few studies have analyzed the predictors of transient and persistent no reflow. In our series, several factors predicted transient no reflow: old age, multi-vessel disease, complex coronary lesion, and stent diameter. In comparison, only old age and pre-procedural TIMI flow 0 predicted the development of persistent no reflow. This suggests that there is a relationship between pre-procedural TIMI flow grade and persistent no reflow, consistent with a prior report.26)
There are several limitations to our study. Despite its prospective, consecutive data collection, this was a non-randomized retrospective analysis which resulted in differences in the baseline clinical and angiographic findings among groups. This study also used a small number of patients with persistent no reflow. Although we performed Cox-regression analysis adjusting 5 variables (age, STEMI diagnosis, Killip class≥3, left ventricular ejection fraction and multivessel disease) to avoid overfitting, the small number of patients in the persistent no reflow group might be related to overfitting in the multivariate analysis. In addition, no information on the use of intracoronary agents to reverse no reflow was available because our registry does not contain this data. Furthermore, confirmation of no reflow might vary among the interventional cardiologists at each participating center, because there is no verification of catheterization laboratory data at every center. Although several studies reported on the importance of a core laboratory to verify coronary flow,27)28) angiographic reperfusion assessment by both an operator and a core laboratory correlated with survival.29) Finally, our registry does not include detailed information on coronary lesion anatomy. Although previous studies identified several coronary anatomy factors related to no reflow, our study was limited in the ability to analyze this association.
In conclusion, this study determined that persistent no reflow in patients with AMI who underwent PCI with coronary stents was associated with poor in-hospital outcomes and increased long-term mortality mainly driven by increased cardiac death despite its low incidence.



 XML Download
XML Download