

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Thromboangiitis obliterans, which is widely known as Buerger's disease, is a nonatherosclerotic inflammatory disease that commonly affects small- and medium-sized arteries in the lower extremities.1) Although the most frequently affected arteries in Buerger's disease are below-the-knee arteries, patients may also present with multilevel arterial occlusive disease.2) Along with strict abstinence from smoking, endovascular revascularization could be a feasible and effective treatment for Buerger's disease patients with critical limb ischemia (CLI).3) However, the success rate of endovascular recanalization in Buerger's disease patients with CLI might be lower, as compared to patients with atherosclerotic peripheral arterial disease. Furthermore, the high rate of in-stent restenosis is a major problem of endovascular treatment.4)5) Surgical recanalization may be an option for the treatment of in-stent occlusion, but it could also be limited due to the lack of potential distal targets in patients with Buerger's disease. Herein, we reported a Buerger's disease patient with multilevel total occlusion extending from the superficial femoral artery to infrapopliteal lesions and limited vascular accesses, who was successfully treated with percutaneous transluminal angioplasty.
Case
A 47-year-old man with a current history of heavy smoking visited our hospital with resting pain and aggravated gangrene in his right 3rd-to-5th toes (Rutherford category 5). By the age of 38, he was diagnosed with Buerger's disease according to the clinical diagnostic criteria and his peripheral angiography showed the typical angiographic findings of corkscrew collateral vessel (Fig. 1).1)6)
He had been treated with endovascular therapy 5 times in the past 10 years. Three years ago, he had also presented with CLI in the same leg, for which, femoropopliteal bypass surgery using an 8-mm Hemashield graft, as well as popliteal artery stenting, were performed. On examination, no arterial pulse was palpable below the common femoral artery level. Computed tomography (CT) angiography showed total occlusion of the entire native femoropopliteal artery, the bypass graft, and below-the-knee arteries (Fig. 2). The previously implanted stent in the right popliteal artery was also totally occluded. The ankle brachial index was 0.56 for the right leg. Surgical recanalization was not eligible due to the lack of distal targets, so an endovascular procedure was planned as an alternative option.
Fig. 1
Angiography of the patient's right lower extremity at the time Buerger's disease was first diagnosed. (A) Proximal part of superficial femoral artery was grossly normal without evidence of atherosclerosis while distal part of superficial femoral artery and popliteal artery were totally occluded with collateral vessels. (B) Below-the knee level angiogram showed total occlusion of popliteal artery, anterior tibial artery, and posterior tibial artery with collateral vessels. (C) Foot level angiogram showed the typical angiographic findings of corkscrew collateral vessel. (D) Final angiogram after endovascular treatment shows that that there was no residual stenosis in femoropopliteal artery.
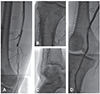
Fig. 2
The patient's lower extremities, as observed via computed tomography angiography. (A) A maximum intensity projection reconstruction image shows total occlusion of the entire native femoropopliteal artery, the bypass graft, and below-the-knee arteries. (B) Axial images; white arrows indicate total occlusion of the surgical bypass graft and the stent that was implanted in the popliteal artery.

By using the antegrade femoral approach with a 6-Fr sheath, angiography revealed the same findings as the CT angiography (Fig. 3).
There was no visible proximal stump of the native superficial femoral artery or the bypass graft. Distal vessels could not be visualized on the angiogram for a potential retrograde vascular access. To overcome this access problem, direct retrograde puncture of the popliteal stent was performed with an 18-gauge puncture needle under fluoroscopic guidance (Fig. 4A). A 0.035-inch hydrophilic guide wire (Terumo, Tokyo, Japan) was gently introduced and advanced through the stent to the level of the proximal femoropopliteal bypass graft. The guide wire, which was supported by a 4-Fr diagnostic Judkins right catheter (Cook Medical, Bloomington, IN, USA), was passed to the common femoral artery and carefully withdrawn through the femoral access using the Rendezvous technique. Once a sufficient length of guide wire was withdrawn through the femoral sheath, the 6-Fr shuttle sheath was advanced over the same guide wire to the previously inserted stent in the popliteal artery after repeated thrombosuction (Fig. 4B). Then, the wire-loop technique with a balloon support was used in a reattempt to crack the occluded in-stent segment in the popliteal artery (Fig. 4C). This time, a 0.014-inch guide wire (Hi-Torque CommandTM, Abbott Vascular, IL, USA) was able to pass through the occluded stent and advance into the posterior tibial artery (PTA) by the subintimal method. After the guide wire was passed through the lesion, balloon angioplasty was performed with a 3.0×250-mm balloon. At that time, the middle part of the 3.0×250-mm balloon was broken at the PTA, because this balloon passed through the previous popliteal stent. Fortunately, the remnant balloon material was successfully retrieved by snare (Amplatz GooseNeck® Microsnare, ev3 Endovascular, Plymouth, MN, USA). Subsequently, balloon angioplasty was done with another 2.5×210-mm balloon in the PTA and dorsal-plantar loop arteries (Fig. 4D), followed by stenting at the proximal anastomosis site of the previous femoral popliteal bypass graft (Fig. 4E).
Fig. 3
Baseline angiography before endovascular treatment showed no visualized distal vessel to access. (A) Total occlusion of the previous femoral popliteal graft. (B) Below-the knee level angiogram showed total occlusion of the popliteal stent, anterior tibial artery, and posterior tibial artery. (C) Foot level angiogram showed total occlusion of the popliteal stent, anterior tibial artery, and posterior tibial artery.

Fig. 4
Step-by-step procedure scheme. (A) Direct retrograde puncture of the previous popliteal stent and advance of the 0.035-inch guide wire. (B) Thrombosuction with the 6-Fr shuttle sheath and an image of the retrieved material. (C) Wire-loop technique with a balloon support. (D) Balloon angioplasty of the posterior tibial artery and dorsal-plantar loop arteries. (E) Stenting at the proximal anastomosis site of the previous femoral popliteal bypass graft.

After complete recanalization of the previous femoral popliteal bypass graft, occluded popliteal stent, and infrapopliteal lesions, final angiography revealed that there was no residual stenosis without any dissection (Fig. 5). A significant improvement in the ankle brachial index for the right leg was observed after the procedure (from 0.56 to 1.00).

Discussion
Although the exact pathophysiology of Buerger's disease is unknown, the inflammatory process is possibly initiated by an unknown intimal antigen. In contrast to atherosclerotic peripheral arterial diseases, Buerger's disease is characterized by the segmental occlusion of not only the distal lower extremity arteries but also the upper extremity arteries.6) The long-term prognosis of patients with Buerger's disease is reported to be significantly worse than that of patients with atherosclerotic peripheral arterial disease. A recent report showed that about 25% of patients are likely to have an amputation, and the risk of amputation increases to 45% after 10 years.7)8) Several clinical diagnostic criteria of Buerger's disease have been suggested, including an age of <45 years, a history of heavy smoking, the presence of distal-extremity ischemia, and exclusion of autoimmune disease, hypercoagulable state, and diabetes mellitus.1) Our patient fulfilled all these criteria at the time Buerger's disease was first diagnosed.
For the treatment of Buerger's disease, surgical revascularization is a reasonable option when bypass is technically feasible. However, surgical treatment for Buerger's disease is often not feasible, due to the lack of distal targets for bypass. Although endovascular treatment may be considered as a therapeutic choice in patients with Buerger's disease, it is also technically challenging because of the diffuse segmental involvement of small distal arteries.9) A small case report series on 17 patients with Buerger's disease showed the clinical benefit of endovascular revascularization in patients with Buerger's disease and CLI.3) With extensive endovascular treatment, technical success was achieved in 95% of patients, and almost 84% of patients had sustained clinical improvement at the time of the 2-year follow-up. In addition, no mortality or complication was observed, and major amputation was not needed.3) Furthermore, with successful revascularization, patients could have an improved quality of life owing to improvements in claudication, resting pain, or wound healing. Nevertheless, in-stent occlusion is also a major problem in the endovascular treatment of patients with Buerger's disease. The therapeutic options to solve this problem are surgical bypass and new endovascular treatment for the occluded stent.
In our patient, revascularization therapy was necessary, due to aggravated gangrene in the toes. Unfortunately, there were no distal targets for bypass, and surgical revascularization was not suitable. A major technical problem was how to gain access for endovascular treatment. By directly puncturing the stent at the popliteal artery, we overcame access difficulty and were able to introduce a guide wire into the intraluminal space. A previous case report showed successful recanalization of occluded superficial femoral artery stents by stent puncture in patients without distal flow.10) In a prospective clinical analysis of diabetics with CLI, the direct stent puncture technique showed a high rate of technical success (98.2%) and clinical success (94.4%).11) Furthermore, it provided favorable clinical outcomes during follow-up periods.11)
In patients with Buerger's disease, endovascular approaches using various techniques should be considered for effective recanalization if a surgical treatment option is not available. For patients with completely occluded stents, direct stent puncture provided easy access to the intravascular space and allowed for successful recanalization to occur without major trauma or fractures of the stent.
In conclusion, the stent puncture technique is a feasible and safe option for overcoming the limitations of vascular access in patients with multilevel total occlusions. Endovascular treatment could be a useful tool for clinically improving CLI in Buerger's disease.
 XML Download
XML Download