

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Large inter-arm difference in blood pressure (BP) is commonly found during physical examination.1) Although the underlying mechanism of such difference is not fully known, the presence of large inter-arm BP difference has been shown to be independently associated with cardiovascular disease and mortality.2) However, previous studies of inter-arm differences have utilized different methodologies to measure BP. To accurately investigate differences in BP between the two arms, both arms must be measured simultaneously and repeatedly using the same device. In previous studies, BP was either sequentially measured,3)4)5)6)7) simultaneously measured with two devices,8)9)10) or measured only once.6)10)11) In addition, most studies were conducted for patients with cardiovascular diseases,5)6)8)11)12)13) with only a few targeting the general populations.3)9)14) Thus, the objective of this study was to examine inter-arm difference in BP among the general population of Koreans and to identify associated factors.
Subjects and Methods
Study population
Data from the Cardiovascular and Metabolic Disease Etiology Research Center (CMERC) cohort that began in 2013 were analyzed in this study. A total of 807 free-living participants residing in four districts (Seoul, Goyang, Gimpo, and Incheon) throughout South Korea between December 2013 and May 2014 were enrolled in the CMERC study. Inclusion criteria were: (1) those who were 30 to 64 years old; (2) those who had lived more than eight months at the current residence without migration plans for the next two years; and (3) those who had ability to provide verbal or written consent to participate in the study. Exclusion criteria were: (1) those who were diagnosed with cancer within the last two years or were currently being treated for cancer; (2) those who had a history of myocardial infarction, stroke, or heart failure; (3) those who were currently involved in pharmaceutical trials; and (4) those who were currently pregnant or with the possibility of being pregnant on the day of registration. All participants completed health questionnaires and health examinations using an identical protocol. After excluding one person with who had missing BP measurements, a cross-sectional analysis was conducted for 806 participants. This study was approved by the Institutional Review Board of Severance Hospital at Yonsei University College of Medicine. All participants provided written informed consent.
Questionnaire data
Standardized questionnaires were used to interview all study participants to acquire information about their demographics, medical history, and health behaviors. Trained interviewers individually carried out the questionnaire surveys according to a predefined protocol. A designated field director double-checked whether the responses were inappropriate or missing. Smoking status was classified into current smoking group and current nonsmoking group (past smoking or never smoking). Alcohol intake was also classified into two groups: current alcohol drinking or current nondrinking (past alcohol drinking or never drinking). Physical activity was measured with International Physical Activity Questionnaire-Short Form, with moderate activity referring to activity that caused individuals to breathe somewhat harder than normal and high activity referring to activity that caused individuals to breathe much harder than normal. Regular exercise was defined as physical activity of moderate-to-high intensity for at least three times per week.
Physical examination
All participants were clothed in lightweight hospital gowns for reliable examinations. Standing height was measured to the nearest 0.1 cm using a stadiometer (DS-102, JENIX, Seoul, Korea). Body weight was measured to the nearest 0.1 kg on a digital scale (DB-150, CAS, Seongnam, Korea) according to a pre-developed protocol. Body mass index (BMI) was calculated as body weight in kilograms divided by standing height in square meters (kg/m2). Waist circumference was measured to the nearest 0.1 cm at the midpoint between the lower border of the rib cage and the iliac crest with an ergonomic circumference measuring tape (SECA 201, SECA, Hamburg, Germany). Mid-arm circumference was measured to the nearest 0.1 cm at the midpoint between the acromion and the olecranon with the right arm hanging (relaxed) using an ergonomic circumference measuring tape (SECA 201, SECA, Hamburg, Germany). Both right and left common carotid arteries were evaluated with B-mode ultrasonography (Accuvix XG, Samsung Medison, Seoul, Korea). During the evaluation, participants were laid in a supine position with their head turning 45° contralateral to the side of scanning. Carotid intima-media thickness (IMT) was measured as the perpendicular distance between the leading edge of the first and second echogenic lines at the far wall of both common carotid arteries.15)16) Max carotid IMT was defined as the highest value of the IMTs of the right and left common carotid arteries.
Laboratory assays
Blood samples from overnight fast participants were collected from the antecubital vein. Enzymatic methods were used to measure the levels of total cholesterol, high-density lipoprotein cholesterol, and triglycerides (ADVIA 1800 Auto Analyzer, Siemens medical Sol., Deerfield, IL, USA). Fasting blood glucose concentrations were measured using a colorimetry method (ADVIA 1800 Auto Analyzer, Siemens medical Sol., Deerfield, IL, USA). Serum insulin concentrations were measured in accordance with the instructions of a radioimmunoassay (SR-300, Stratec, Birkenfeld, Germany). Hemoglobin A1c (HbA1c) concentrations were measured with high performance liquid chromatography (Variant II TURBO, Bio-Rad, Berkeley, California, USA) according to the National Glycohemoglobin Standardization Program. Uric acid concentrations were measured using a colorimetry method (ADVIA 1800 Auto Analyzer, Siemens medical Sol., Deerfield, IL, USA). C-reactive protein (CRP) concentrations were determined using a turbidimetric immunoassay (ADVIA 1800 Auto Analyzer, Siemens medical Sol., Deerfield, IL, USA).
Blood pressure measurements
Brachial BP was measured for both arms using an automated oscillometric device (WatchBP office, Microlife, Widnau, Switzerland) equipped with two cuffs for simultaneous double-arm measurements. Cuff size was tailored to the arm of an individual according to their mid-arm circumference. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were repeatedly measured after at least five minutes of rest in seated position. The average of the three measurements was used in analysis. Differences in BP were calculated by subtracting the left-arm BP (L) from the right-arm BP (R). Absolute BP difference or absolute value of R–L (|R–L|) was calculated to determine the difference between left arm BP and right arm BP regardless of which arm showed higher BP value. A large inter-arm BP difference was defined as an absolute inter-arm BP difference of greater than 10 mmHg.17) Hypertension was defined as SBP≥140 mmHg, DBP≥90 mmHg, or currently under treatment with anti-hypertensive medications. Prehypertension was defined as SBP≥120 mmHg or DBP≥80 mmHg.
Statistical analysis
Differences in general characteristics and variables of interest between men and women were evaluated. Continuous variables were described as mean and standard deviation for normally distributed variables or as median and interquartile range for skewed variables. Differences in continuous variable and normally distributed variables were tested by independent t-test and Wilcoxon rank sum test, respectively. Categorical variables were described as numbers (percentages) and tested by chi-square tests. General characteristics and concentrations of selected biomarkers were analyzed according to inter-arm BP difference. The relationship between inter-arm BP difference and other variables were evaluated using Pearson’s correlation coefficients. To identify factors independently associated with inter-arm BP difference, adjusted odds ratios (OR) and 95% confidence intervals (CIs) were calculated using multivariate logistic regression models including age, sex, BMI, CRP, mean SBP, and anti-hypertensive medications. The above analyses were repeated after excluding participants taking anti-hypertensive medications in sensitivity analysis. All statistical analyses were performed using SAS version 9.2 (SAS Institute, Cary, NC, USA). Statistical significance was considered when two-sided p was less than 0.05.
Results
The general characteristics of the study participants are summarized in Table 1. The study participants included 237 men with a mean age of 50.2 years and 569 women with a mean age of 51.2 years. The mean SBP and DBP of all participants were 115.0 and 73.5 mmHg, respectively. The mean absolute inter-arm differences in SBP and DBP were 3.3 and 2.0 mmHg, respectively. The proportion of hypertension and prehypertension were 21.2% and 25.8%, respectively.
Table 1
General characteristics of study participants
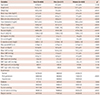
Data are presented as means±standard deviation, median [inter quartile range], or numbers (percent). *p was derived from independent t-test, Wilcoxon rank sum test, or chi-square test. HDL-C: high-density lipoprotein cholesterol, IMT: intima-media thickness, SBP: systolic blood pressure, DBP: diastolic blood pressure, PP: pulse rate
The distribution of right-to-left BP differences is shown in Fig. 1. Overall, SBP and DBP in the right arm were 0.7 and 1.1 mmHg higher than that in the left (SBP: p=0.114; DBP: p=0.013). In 50.9% of the participants, SBP in the right arm was higher than that in the left arm. In 37.6% of the participants, SBP in the right arm was higher than that in the left arm. In the remaining 11.5% of participants, SBP in the right arm was the same as that in the left arm. Regarding the DBP, 58.3% of participants had higher DBP in the right arm than that in the left arm, 24.1% of participants had lower DBP in the right arm than that in the left arm, while the remaining 17.6% of subjects had the same DBP in the right arm and the left arm. The right SBP was correlated with the left SBP (r=0.95, p<0.001). The right DBP was also correlated with the left DBP (r=0.96, p<0.001, data not shown).
Fig 1
Distribution of inter-arm blood pressure differences. (A) Inter-arm SBP difference (right-left), mmHg. (B) Inter-arm DBP difference (right-left), mmHg.
SBP: systolic blood pressure, DBP: diastolic blood pressure.

The distribution of absolute inter-arm BP differences is shown in Fig. 2. Absolute inter-arm differences≥10 mmHg in both SBP and DBP were found in 30 (3.7%) and 7 (0.9%) participants, respectively. However, the frequency of an absolute inter-arm SBP≥10 mmHg was 3.0% in people with normal BP, and 6.4% in people with hypertension (p=0.060, data not shown).
Fig 2
Distribution of absolute values of inter-arm blood pressure differences. (A) Absolute inter-arm SBP difference, mmHg. (B) Absolute inter-arm DBP difference, mmHg. SBP: systolic blood pressure, DBP: diastolic blood pressure.

The characteristics of study participants according to inter-arm difference in BP are summarized in Table 2. Participants with large inter-arm SBP differences had higher weight, higher waist circumference, higher concentration of uric acid, higher CRP level, and higher BP compared to other participants. Participants with large inter-arm DBP difference had higher weight, higher BMI, bigger waist circumference, bigger mid-arm circumference, and higher CRP level compared to other participants.
Table 2
General characteristics of study participants according to inter-arm blood pressure differences
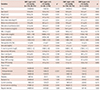
Data are presented as means±standard deviation, median [inter quartile range], or numbers (percent). *p was derived from independent t-test, Wilcoxon rank sum test, or chi-square test. SBP: systolic blood pressure, DBP: diastolic blood pressure, HDL-C: high-density lipoprotein cholesterol, IMT: intima-media thickness, PP: pulse rate
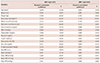
The correlations between absolute inter-arm BP difference and other variables are summarized in Table 3. An absolute inter-arm difference in SBP was positively associated with height, weight, BMI, waist circumference, mid-arm circumference, triglycerides, uric acid, CRP, max carotid IMT, and BP. Meanwhile, an absolute inter-arm difference in DBP was positively associated with weight, BMI, waist circumference, mid-arm circumference, triglycerides, fasting glucose, HbA1c, CRP, and BP.
Table 3
Correlation between inter-arm blood pressure difference and anthropometric or clinical characteristics
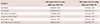
Factors associated with inter-arm BP difference≥10 mmHg were assessed by multivariate logistic regression models, including age, sex, BMI, CRP, mean SBP, and anti-hypertensive medications (Table 4). An inter-arm difference of SBP≥10 mmHg was independently associated with mean SBP (OR: 1.04 per mmHg; 95% CI: 1.02-1.07) and CRP (OR: 1.05 per mg/L; 95% CI: 1.01-1.09). An inter-arm difference of DBP≥10 mmHg was only independently associated with BMI (OR: 1.33 per kg/m2; 95% CI: 1.06-1.67). In sensitivity analysis excluding participants taking anti-hypertensive medications, a large inter-arm difference in SBP was independently associated with mean SBP (OR: 1.05 per mmHg; 95% CI: 1.02-1.08) and CRP (OR: 1.04 per mg/L; 95% CI: 1.01-1.09). A large inter-arm difference in DBP was only independently associated with BMI (OR: 1.41 per kg/m2; 95% CI: 1.08-1.84; Supplementary Table 1 in the online-only Data Supplement).
Table 4
Factors associated with large inter-arm difference in blood pressure
Discussion
The present study investigated the distributions of inter-arm differences in BP for the general Korean population and identified their associated factors. Large inter-arm differences≥10 mmHg in SBP and DBP were found in 3.7% and 0.9% of participants, respectively. A large inter-arm difference in SBP was independently associated with mean SBP and CRP, while a large inter-arm difference in DBP was only independently associated with BMI. To our knowledge, the current study is the first to investigate the distribution of inter-arm BP differences and identify the factors associated with large inter-arm difference in the general population of Koreans. Most previous studies have examined the distribution of inter-arm BP differences in patients with risk factors of cardiovascular disease,18)19)20) the association between inter-arm BP differences and cardiovascular disease in patients with hypertension,5)10)12)21) or the association between inter-arm BP differences and mortality in patients with cardiovascular diseases.6)11) Only a few studies have been conducted for the general population.3)9)14) In a Ohasama study14) in Japan, the proportion of participants with an absolute inter-arm SBP difference≥10 mmHg was 9.1%. A large absolute inter-arm difference in SBP was found to be independently associated with BMI, HbA1c, ankle brachial index, hypertension, and hypercholesterolemia. In a Framingham Heart Study3) in USA, absolute inter-arm differences of SBP≥10 mmHg were noted in 9.4% of participants. In their study, inter-arm SBP difference was associated with significantly increased risk for future cardiovascular events after 13.3 years. In a Hypertension Genetic Epidemiology Network study with hypertensive siblings and volunteers recruited separately, the proportion of absolute inter-arm SBP difference≥10 mmHg was 14.2% and 9.2% in the two groups (hypertensive siblings and volunteers), respectively.7)
The prevalence of a large inter-arm difference in BP in this study was lower than that in previous studies.3)14) This might be due to differences in study populations and methods used for BP measurement. For example, the participants used in this study were younger than those used in the Framingham Heart Study3) or the Ohasama study14) (61.1 or 62.4 vs. 50.9 years). In addition, our study participants had lower prevalence of hypertension compared to the other two studies (21.2 vs. 50.1 or 42.3%). We simultaneously measured BP for both arms three times in seated position using an automated device. However, the Ohasama study14) simultaneously measured BP for both arms only two times in supine position, while the Framingham Heart Study3) sequentially measured BP three times in supine position. According to the American Heart Association, the European Society of Hypertension, and the European Society of Cardiology guidelines, BP should be repeatedly measured in seated position to acquire accurate BP values.22)23) In a recent meta-analysis, the relative risk (RR) of obtaining an inter-arm SBP difference≥10 mmHg was higher when BP was measured sequentially instead of simultaneously (RR: 2.2; 95% CI: 1.4–3.6) and when performing only one BP measurement was used instead of multiple measurements (RR, 2.0; 95% CI, 1.1–3.8).24) Heart rate variation can contribute to BP variations. The inter-arm BP difference measured non-simultaneously not only reflects the true difference between arms, but also random fluctuation due to heart rate variation.25) Single or multiple measurements can also affect the observed inter-arm differences in BP. When an individual’s BPs are measured multiple times, later BP values tend to be lower than earlier values. Inter-arm BP differences also tend to be smaller in later measurements.26) In the present study, we calculated inter-arm differences using the average of three serial measurements of BP. In our analysis, inter-arm BP difference at the second or third measurements tended to be smaller than the difference at the first measurement. In addition, inter-arm BP difference based on multiple measurements was even smaller than the inter-arm difference at the last single measurement (Supplementary Table 2 in the online-only Data Supplement). This finding implies that a single measurement of BP might overestimate an individual’s inter-arm BP difference compared to multiple measurements of BP.
Our results revealed that the right arm BP was higher than the left arm BP, which was in consistent with results of previous studies.4)14)27) A possible explanation is that muscles in the dominant arm are more developed that it might take more pressure in the right arm cuff to overcome tissue inertia. Hence, BP in the right arm of right handed people might be measured higher than the BP in their left arm.4) In addition, slight differences of anatomical structures such as angulation and branching of the aorta as well as hemodynamic profiles might have affected the result.28)
In our study, a large inter-arm difference in SBP was independently associated with CRP and mean SBP while a large inter-arm difference in DBP was independently associated with BMI. These findings are in consistent with results of several previous reports. In a USA cohort study of hypertensive patients, elevated CRP concentrations have been more frequently found in patients with large inter-arm difference in SBP (≥15 mmHg) compared with those with normal inter-arm SBP differences (53% vs. 33%).13) Since CRP is related to subclinical atherosclerosis and local atherosclerotic subclavian obstructions increase BP differences between the two arms, an association of elevated CRP with inter-arm BP difference can be expected.29) Several studies have reported the association between hypertension and inter-arm BP differences, including the Framingham Heart Study,3) a Finrisk 2007 study/DILGOM-study,9) a Kaohsiung Municipal Hsiao-Kang Hospital study of Taiwan,10) the Ohasama study,14) and a primary medical care study in Japan.21) Several studies have also reported the association between BMI and inter-arm BP differences, including the Kaohsiung Municipal Hsiao-Kang Hospital study of Taiwan,10) the Ohasama study,14) and the primary medical care study of Japan.21) The present study has several limitations. Firstly, this study had a relatively small sample size. Therefore, we could not conduct sub-group analyses according to sex or age groups. Secondly, this study was conducted as a cross-sectional study in which all information was collected at the same time point. Therefore, we could not investigate risk factors causing increases in inter-arm BP differences. Thirdly, we could not exclude individuals with subclavian stenosis because data for angiography or imaging studies were unavailable. Fourthly, even though we measured BP three times, all BP measurements were done in a single day in an office setting. Therefore, these values may not represent BP status on a typical day.
In conclusion, large inter-arm BP differences were only present in a small portion of healthy Korean adults. Our findings suggest that high SBP, chronic inflammation, and obesity might be associated with larger inter-arm differences in BP.
 XML Download
XML Download